Apocrine carcinoma comprises a group of rare primary cutaneous
carcinomas (a subtype of sweat gland carcinoma), which show features of apocrine differentiation.
Frequently they are
indolent and slowly developing, but some are rapidly progressive and
aggressive
. Wide, local excision with clear
margins, with or without lymph node dissection is the standard
treatment.
It occurs mostly in
apocrine-dense regions such as the axilla and anogenital areas, although
it has also been reported to occur in less typical locations such as the
nipple, scalp, forehead, ear canals, trunk, wrists, feet, toes, and
fingers.
Rarely, the tumour may arise in the Moll’s glands of the eyelids.
Tumours arising from the anogenital region are regarded as carcinomas of
the anogenital glands by some pathologists.
Slow growing lesions can be present as
painless, solitary, or multiple, solid to cystic masses,
ranging in size from 1 to over 5 cm.
Colour may vary from red to purple, and show ulceration of the
overlying skin.
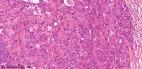
Non-encapsulated, infiltrative tumour
located in the lower dermis and subcutaneous tissue and consists of
multiple ductal structures ;
Different growth patterns include papillary, tubular, cribriform, cord-like and solid ;
Eosinophilic cells with granular and sometimes
vacuolated cytoplasm ;
At least focal decapitation secretion
;
Variable mitotic activity and pleomorphism ;
Normal or hyperplastic apocrine glands
are often identified close to the
invasive tumour ;
Cells contain PAS-positive, diastase resistant granules
;
Hemosiderin granules may be present in the cytoplasm.
Non-encapsulated, infiltrative tumour
located in the lower dermis and subcutaneous tissue and consists of
multiple ductal structures ;
Different growth patterns include papillary, tubular, cribriform, cord-like and solid ;
Eosinophilic cells with granular and sometimes
vacuolated cytoplasm ;
At least focal decapitation secretion
;
Variable mitotic activity and pleomorphism ;
Normal or hyperplastic apocrine glands
are often identified close to the
invasive tumour ;
Cells contain PAS-positive, diastase resistant granules
;
Hemosiderin granules may be present in the cytoplasm.
Tumour cells usually express cytokeratin, epithelial membrane antigen
and gross cystic disease fluid protein-15.
Carcinoembryonic
antigen is usually negative.
Some cases demonstrate positivity with S100
protein.
The tumours are initially locally invasive, and systemic
dissemination is often associated with regional lymph node
metastases.
Wide, local excision is the standard treatment for
such lesions.
Adjuvant radiotherapy may be used in cases with advanced local
or regional lesions.
Differential diagnosis:
Metastatic breast
carcinomas may be indistinguishable; Eccrine ductal
carcinoma.
Dermatopathology Quiz Case
6 |