

Custom Search
|


| Dermpath-India Pathology of Atypical Fibroxanthoma Dr Sampurna Roy MD 2022
|
|
-Atypical fibroxanthoma (AFX) is a tumour of older adults, arising in actinically damaged skin, almost exclusively in the head and neck area -AFX is usually a pleomorphic tumor, although a spindle cell variant is also recognized -AFX does not infiltrate the subcutaneous fat and does not exhibit necrosis, vascular invasion, or perineural invasion -AFX is a diagnosis of exclusion; sarcomatoid carcinoma, melanoma, and leiomyosarcoma must be excluded -AFX is benign and does not metastasize
|
The term 'Atypical Fibroxanthoma', was introduced by Helwig EB (Texas J Med 1963;59: 664-667 ). Similar cases were reported as Paradoxical fibrosarcoma of the skin or pseudosarcoma by Bourne RG (Med J Aus 1963;1:5 04-510).
- The tumour usually presents as solitary, rapidly growing dome shaped ulcerated and crusted nodule, usually less than 2 cm in diameter, on the head or neck region of the elderly.The lesion usually occurs in sun-damaged or radiation damaged skin.
- A rare clinical variant occurs in younger patients. The tumour is
larger and slow growing and are usually located on the trunk and
extremities.
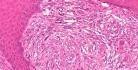
- Located in the dermis. - Expansile growth. The tumour is usually bordered by mononuclear inflammatory cells in the deeper aspect. - The adjacent adnexal structures are usually compressed. Adnexal structures within the tumour are always intact. - The overlying epidermis is thin and usually ulcerated with crust formation, but there may be peripheral epidermal acanthosis with formation of 'epithelial collarette'. - A thin grenz zone may be present separating the tumour from the epidermis or the tumour may stream out from the basal layer. In the latter case the dermo-epidermal junction is not always clear. - The tumour is characterized by marked pleomorphism and polymorphism .
- There is an admixture of three main cell types: Note: Oil red O stain on frozen sections show variable amount of lipid in the polyhedral and giant cells. - Typical and atypical mitotic figures are noted (one per high power field). - The epidermis overlying the tumour usually do not show evidence of atypia, junctional activity or atypical melanocytes. However, epidermis adjacent to the tumour may show evidence of actinic keratosis. - Dermis adjacent to the main lesion show features of solar elastosis. Telangiectatic blood vessels may be present near the surface. - In rare cases foci of osteoid and chondroid differentiation and osteoclast like giant cells may be present. - Spindle cell variant is entirely composed of monomorphic palely eosinophilic spindle shaped cells arranged in fascicles. There is only mild pleomorphism. (Differential diagnosis: leiomyosarcoma, spindle cell squamous carcinoma and spindle cell melanoma). Histologic variants of Atypical Fibroxanthoma : Spindle cell ; Clear cell ; Osteoclastic ; Chondroid ; Pigmented ; Granular cell; Following features help to exclude Atypical Fibroxanthoma from other lesions: 1. Presence of vascular and / or perineural invasion. 2. Extensive necrosis away from the ulcerated surface. 3. Extensively infiltrative growth pattern. 4. Deep extension into the subcutaneous fat. Immunohistochemical features: Vimentin shows diffuse strong cytoplasmic positivity. Smooth muscle actin shows focal but strong cytoplasmic staining in many cases. Alpha1- antitrypsin, alpha1- antichymotrypsin, HAM56 (non-specific) are immunopositive. CD68 (monocyte-macrophage marker) shows some positivity. CD74 is weakly positive in some cases. (In undifferentiated pleomorphic sarcoma CD74 is strongly positive). In a few cases scattered cells stain positively for factor XIIIa. Focal positivity for CD99 has been reported. Differential diagnosis of Atypical Fibroxanthoma: 1. Spindle Cell Squamous Cell Carcinoma: Infiltrative tumour and overlying epidermal dysplasia is present. Cytokeratin is positive. 2. Malignant melanoma: S100 protein and HMB45 positive. Spindle cell melanomas are usually amelanotic,infiltrative tumour with uniform cytology and are often associated with desmoplasia. Neural invasion may be present. 3. Leiomyosarcoma: Infiltrative, poorly circumscribed tumour composed of bundles of spindle cells. Primary cutaneous leiomyosarcoma shows minimal cytological atypia. Metastatic tumours are well circumscribed and demonstrates prominent cellular atypia. Desmin is positive. Note: Immunohistochemical analysis is absolutely essential to confirm the diagnosis. 4. Undifferentiated pleomorphic sarcoma: Deep soft tissue tumour. CD74 is strongly positive. 5. Dermatofibrosarcoma protuberance: Characteristic monomorphic cytology, storiform arrangement. 6. Reticulohistiocytoma: Composed of epithelioid cells with 'ground glass' cytoplasm. 7. Post irradiation: Features similar to atypical fibroxanthoma may be present in post irradiated skin.
|
|
|
