

Custom Search
|


|
Custom Search
|
|
Dermpath-India Pathology of Chondroid Syringoma Dr Sampurna Roy MD 2023
|
 |
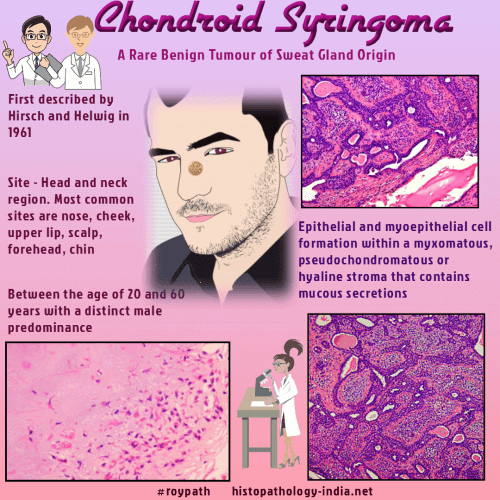
| Chondroid syringoma
represents the cutaneous counterpart of mixed tumor ("pleomorphic
adenoma") of salivary glands, therefore it is also termed 'mixed tumour of
the skin'.
The cutaneous lesion has different behaviour in that it rarely
recurs even if inadequately excised. Age:
Usually occurs in middle aged and elderly patients.
Head and neck region and rarely in the distal extremities. The tumour presents as a solitary, slow growing nodule (0.5 - 3 cm in diameter).
Hyaline cell-rich chondroid syringoma :- Histopathological features: Lobulated neoplasm composed of hyaline cells with plasmacytoid features showing ovoid nuclei, with occasional invaginations, finely granular chromatin, and discrete nucleoli; the cytoplasm is deeply eosinophilic with occasional dot-shaped paranuclear hyaline inclusions ; Hyaline cells might possess an aberrant myoepithelial differentiation; Immunohistochemistry: Hyaline cells are strongly and diffusely positive for S-100 protein, pan and high molecular weight cytokeratins. Cells are focally positive for GFAP, neuron-specific enolase, and cytokeratin 14. Differential diagnosis: Malignant melanoma and extra-skeletal myxoid-chondrosarcoma. Atypical mixed tumours:- Borderline features of malignancy characterized by an infiltrative margin, satellite tumour nodules, and tumour necrosis . These tumours do not metastasize. Malignant chondroid syringoma:- A few cases have been reported; More common in women ; Occurs most often in trunk and extremities ; May metastasize to both the regional and distant lymph nodes, causing the death of the patient. In these cases, radiation therapy follows the surgical excision. Microscopic features: Lobulated appearance ; Composed of epithelial and mesenchyme-like component (myxomatous and cartilaginous areas) ; Epithelial component predominates at the periphery of the tumour; Mesenchymal component is at the center; Scattered mitoses ; Variable pleomorphism. Immunohistochemistry: Positive staining for cytokeratin, S-100 protein, neuron- specific enolase and glial fibrillary acidic protein.
|
|
|
|
|
Visit:-
Infectious Disease Online
 Prof (Dr) Haradhan Roy MD (AIIMS) (1928-2022) (R) Director-Professor and Head of the Dept of Pathology, Calcutta National Medical College, Calcutta University India |

Consultant Histopathologist (Kolkata - India)
|
![]()
Copyright ©
2002-2023 histopathology-india.net