

Custom Search
|

|
Infectious Disease Online Pathology of Coccidioidomycosis (Valley Fever) |
|
Coccidioidomycosis is caused by
the dimorphic fungus Coccidioides immitis.
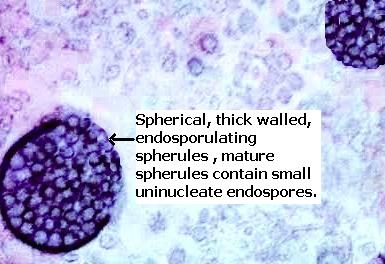
The organism is thick-walled, mature, spherules containing endospores. Spherules rupture liberating endospores into surrounding tissue. It causes chronic, necrotizing lesions that clinically & pathologically resembles tuberculosis. High risk groups are African-Americans and Asians, pregnant women during the third trimester, and immunocompromised persons. Construction or agricultural workers, and archeologists who are exposed to dust are also at risk. Epidemiology: Endemic in the south-western United States, parts of Mexico and South America. Reservoir : Soil in semiarid areas.
Mode of infection: Inhalation of airborne arthroconidia (barrel shaped infectious units) from contaminated soil. The contaminated soil may be disturbed following excavation or after a natural disaster like dust storm or earthquake. Arthroconidia mature to form endospore containing spherules. Presentation: A- 60% of air born infections are asymptomatic. B- 40% cases are symptomatic. Lung: Primary pulmonary coccidioidmycosis are acute disease with influenza-like symptoms associated with suppurative or granulomatous pneumonitis with abundant organisms. Initially, there is a solitary area of consolidation, sometimes diffuse pneumonic consolidation or multiple foci of consolidation is seen. Cavitation is the most common complication, which may communicate with bronchial tree. Hilar lymph nodes may or may not be involved. Disseminated lesions (0.5-1% of patients) by hematogemous route are seen in meninges, skin, soft tissue, bones, adrenals, spleen, liver. Meninges: Central nervous system is affected in 50% patients with disseminated lesion. Coccidial meningitis is a chronic lesion with insidious onset. Granulomatous and suppurative lesions are noted affecting basilar process and sometimes brain parenchyma and spinal cord. Hydrochephalus is a complication. Skin: Primary infection is very rare following inoculation of organisms at sites of trauma. In disseminated disease the skin lesions takes the form of verrucous plaques (nasolabial fold), granulomatous papules and nodules usually on the head. Subcutaneous abscesses or pustular lesions and sinus tracts are also noted. Joints: Synovitis and effusion. Usually knee, ankle and wrist joints are involved. Bones: Chronic osteomyelitis. Long bones as well as bones of hands, feet, pelvis and skull may be involved. Other organs involved include: Thyroid, gastrointestinal tract, genito-urinary tract, pericardium and peritoneum Microscopic features: In tissue the inflammatory reaction is both purulent and granulomatous. Endospores incite a polymorphonuclear response. As the endospores mature into spherules, the acute reaction is replaced by lymphocytes, plasma cells, epithelioid cells and giant cells. Lungs: Caseative pulmonary granuloma (resemble Tuberculosis), Epithelioid cells and giants cells may be noted, Organisms are present within the granuloma, Mature spherule with endospores, Hyphae may be present in the pulmonary cavities, Often associated with microabscess formation, Most of the lesions are healed by fibrosis & calcification. Skin: Non caseating granuloma in the upper and mid- dermis, Thick walled spherules within the granuloma, Early lesions and subcutaneous abscesses demonstrate abundant neutrophil polymorphs, Some lymphocytes, histiocytes and eosinophils are also present. Laboratory diagnosis: 1. Skin test ; 2. Serodiagnosis ; 3. Immunoflourescence- confirmatory. |


|
|
