

Custom Search
|


|
Dermpath-India Pathology of Desmoplastic Fibroblastoma (Collagenous Fibroma)
|
|
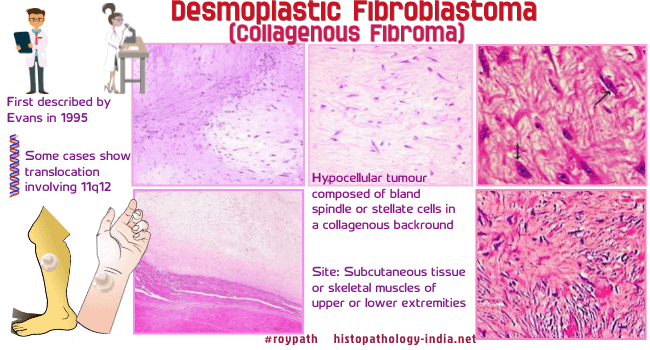
Desmoplastic Fibroblastoma is
a distinctive benign fibrous soft tissue tumour that was first
described by Evans in 1995. Clinical presentation: The lesion presents as a firm, well circumscribed, painless mass of long duration and are commonly located in the subcutaneous tissue or skeletal muscle of upper and lower extremities in adults. Collagenous fibroma has a peak incidence in the fifth to seventh decades of life, with a male predominance. The tumours range in size from 1 to 20 cm. Site: This entity has been reported in various locations, including the upper extremities, posterior neck, upper back, lower extremities, abdominal wall, and hip. Cases have been described in the tongue, lacrimal gland, parotid gland and palate. Gross: Macroscopically, the lesion presents as an elongated, lobulated, or disc-shaped mass with a firm consistency and a homogeneous grayish-white colour. Some cases show translocation involving 11q12. Microscopic features: The tumour is relatively hypocellular. There is proliferation of bland spindle or stellate shaped cells embedded in a fibromyxoid to densely fibrotic collagenous stroma. The stroma may contain a large amount of mucin which is positive with alcian blue. Mitotic figures are very rare or absent, tumour necrosis is not seen, and vascularity is low. The tumour often focally infiltrate the surrounding skeletal muscle and adipose tissue. Immunohistochemistry: Diffusely positive for vimentin. In some cases there may be focal staining for smooth muscle actin. S-100 protein, EMA , CD34, desmin and keratin are usually negative. Electron microscopy: Revealed features consistent with a fibroblastic or myofibroblastic lineage. Differential diagnosis: Fibromatosis- Collagenous fibroma should be differentiated from fibromatosis, which has a high risk of local recurrence if simple local excision is done. Fibromatosis is more cellular and shows short fascicular arrangements of tumour cells and greater infiltration at the periphery than collagenous fibroma. Neurofibroma; Nodular fasciitis ; Fibroma of tendon sheath ; Solitary fibrous tumour; Perineurioma ; low-grade fibromyxoid sarcoma. The tumour does not recur after complete surgical excision.
|
|
|
