

Custom Search
|

|
Infectious Disease Online Pathology of Dermatophytosis
|
|
|
|
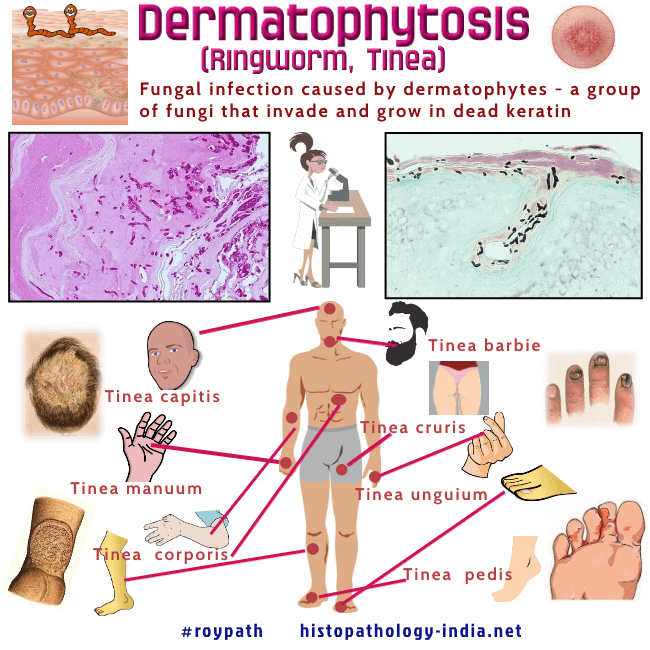
Dermatophytosis is a term used to
describe mycotic infections caused by a group of fungi that usually
remain localized to the superficial layers of the skin, hair, or nails.
This clinical entity is caused by a group of related filamentous fungi - Dermatophytes, of the genera Epidermophyton, Microsporum and Trichophyton. Diseases produced by the dermatophytes occur worldwide and are known as tinea or ringworm. The clinical appearances are variable and depend on a number of factor: (i) Species of fungus (ii) Site of infection (iii) Immunological status of the patient (iv) Use of topical steroid. Atypical presentation following use of topical steroids have been called 'tinea incognito'. Generally, clinical manifestations include itching, a ring-shaped rash, skin that appears red, scaly, or cracked, and hair loss. The symptoms usually appear 4–14 days after the body comes in contact with the pathogenic fungi. Subtypes: - Tinea Capitis: ( tinea of the head , scalp, eye-brow, and eyelash). Kerion is a boggy violaceous inflammatory area of dermal suppuration and folliculitis. Favus is a chronic infection of the scalp and rarely of the glaborous skin which is usually acquired in childhood. - Tinea Faciei : Rare variant presenting as a facial erythema with scaling - Tinea barbae is the name used for infection of the beard and moustache areas of the face with dermatophyte fungus. - Tinea corporis (nonhairy skin): Is a superficial fungal skin infection of the body. It is defined explicitly by the location of the lesions that may involve the trunk, neck, arms, and legs. The term 'radiation port dermatophytosis' is used for cases of tinea corporis localized to irradiated skin. - Tinea cruris (of the groin/inguinal region): Occurs exclusively in males. Have been noted in patients with AIDS. Diaper dermatitis is a variant which predominantly affects infants. -Tinea Pedis (of the foot - athlete's foot): Common in swimmers. -Tinea unguium (Onychomycosis) : Fungal infection of the nail. The lesion presents as thickening, discoloration, and deformity of the nails. Fungal organisms are present in the deeper portions of the nail plate and in the hypertrophic nail bed. PAS- stain is used to demonstrate the fungal elements. - Majocchi's granuloma: It is common in females and often occurs in immunocompromised patients. The lesion presents as nodular and plaque-like lesions of the lower leg. Microscopic features are of granulomatous perifolliculitis. The nodular granulomatous lesions in the dermis contain individual dermatophyte hyphae. - Tinea Manuum: Infection of skin of palmar aspect of hand. Microscopic features:
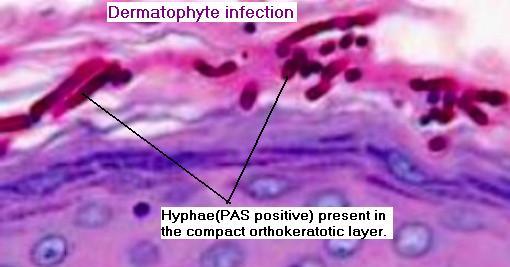
Note the "sandwich sign" where the hyphae are sandwiched at the interface between normal and abnormal layers of cornified cells" Dermatophyte infection may display a wide range of microscopic features. Changes in stratum corneum include: (i) Presence of neutrophils; (ii) Compact orthokeratosis ; (iii) Presence of 'Sandwich Sign' - Characterized by hyphae sandwiched in between an upper normal basket weave stratum corneum and lower layer of abnormal stratum corneum - (compact orthokeratotic or parakeratotic in type). Epidermis may show: Mild spongiosis ; Prominent spongiotic vescicles (palms and soles) ; Rarely subcorneal or intraepidermal pustules ; Chronic cases show variable acanthosis. Dermis may show sparse perivascular mixed inflammatory infiltrate or a heavy dermal infiltrate with involvement of hair follicle. Perifollicular neutrophils or a mixed inflammatory infiltrate may be present. Dermatophytes are identified in the tissue as branched, septate hyphae and spores. They usually stain with hematoxylin and eosin but are best demonstrated with special stains for fungi. Hyphae and arthroconidia invade the stratum corneum, hair follicle and hair shafts. The pattern of hair invasion may be ectothrix, endothrix or endoectothrix. Occasionally, rupture of a hair follicle and release of fungal elements into the dermis elicits acute suppurative inflammation that eventually becomes granulomatous. Aggregates of hyphae embedded in and surrounded by abundant Splendore - Hoeppli material in the dermis and subcutaneous tissue may be misinterpretated by some pathologists as grains and granules found in Mycetoma. The aggregates actually consist of clustered dermatophyte hyphae (pseudogranules) each ensheathed by Splendore- Hoeppli material. Note: The presence of hyphae in the very thin compactly orthokeratotic zone in the lowermost part of the stratum corneum of a section stained by hematoxylin and eosin is diagnostic of dermatophytosis.
|
|
|
