

Custom Search
|

|
Infectious Disease Online Pathology of Diphtheria
|
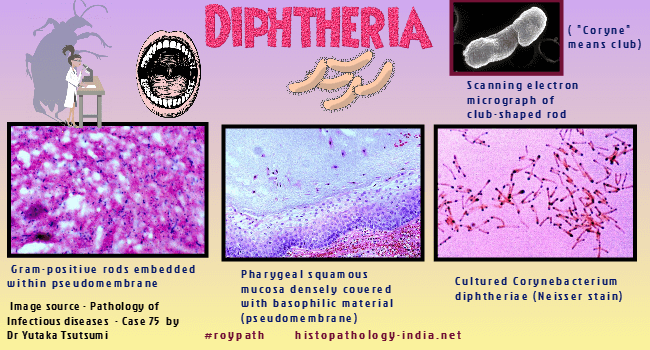
Diphtheria is an acute disease that results from a localized infection and a systemic toxemia caused by exotoxin producing strains of Corynebacterium diphtheriae. The name is derived from the Greek words koryne (club) and diphtheria (leather), the latter referring to the grey membrane at the site of infection. It is possible to completely eradicate Diphtheria by routine immunization with diphtheria toxoid. Even in medically advanced countries, however, diphtheria may occur when immunization procedures breakdown because of war or complacency. An important epidemic occurred in Texus in 1970. The low-grade endemicity of diphtheria depends on the occurrence of toxigenic Corynebacterium diphtheriae in the nasopharynges of a small number (fewer than 1%) of asymptomatic human carriers. Transmission to nonimmune individuals usually occurs by the respiratory route. In diphtheria, unlike food poisoning or tetanus, a parasitic relationship exists between the causative microorganism, Corynebacterium diphtheriae, and its host. Clinical Presentation: Diphtheria is a composite of a local inflammation and a systemic intoxication. Toxin produced locally by toxogenic strains of Corynebacterium diphtheriae is responsible for an inflammatory reaction on body surface at the site of infection (usually the oral pharynx, from which the process often extends to the nose or larynx). Occasionally the tracheal, esophageal, or gastric mucosa is involved as well. Less commonly, but particularly in the tropics, cutaneous trauma or burns may be the site of diphtheria. The umbilical cord (in diphtheria neonatorum), the genital tract, and the conjuctivae are rare sites. Unlike streptococcal tonsilitis, diphtheria is often insidious in onset and may be preceded by 2 to 3 days of listlessness, malaise, and headache before local symptoms occur. Cervical adenopathy seems out of proportion to the pharyngeal lesion. Soon small gray or white patches of exudates appear on the pharyngeal mucosa, usually over the tonsils. These enlarge and coalesce and, with the accumulation of blood, become gray or black. This exudate constitutes the characteristic diphtheritic membrane, which consists of leukocytes and numerous bacteria enmeshed in a dense network of fibrin. The epithelial surface becomes necrotic and densely adherent to the overlying membrane. This adherence explains why raw bleeding points are exposed when the membrane is forcibly removed. If particularly extensive cases, the local process may produce mechanical respiratory obstruction, stridor, and even asphyxiation. The local inflammatory process and its mechanical consequences are less important in the evolution of diphtheria than is the profound toxemia that characterizes the infection. Diphtheria toxin, produced by Corynebacterium diphtheriae in response to infection of that organism by a specific bacteriophage, is a potent inhibitor of cellular protein synthesis. It is readily absorbed from the point of production into the blood stream, and its effects are noted in many organs and systems throughout the body. Clinically, apparent weakness or paralysis of limbs is rare. Neuropathic manifestations of diphtheria are usually temporary and disappear within 2 or 3 months if the patient survives.
|
![]()
Copyright © 2022 histopathology-india.net