

Custom Search
|

|
Infectious Disease Online Pathology of Echinococcosis (Hydatid Disease)
|
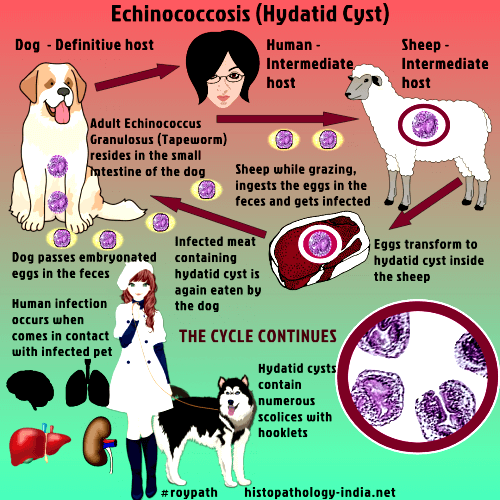
Echinococcosis or hydatidosis, in humans is a zoonotic infection caused by larval stages (metacestodes) of cestode species of the genus Echinococcus. Echinococcus granulosus causes cystic hydatid disease. Echinococcus multilocularis causes alveolar hydatid disease. Echinococcus vogeli or Echinococcus oligarthrus is the cause of polycystic hydatid disease , a disease with features similar to those of alveolar hydatid disease. Areas of high incidence: East Africa include East Africa, Spain, Greece, the Middle East, Iran, western Australia, Chile, Argentina, and Uruguay. Echinococcus multilocularis causes alveolar hydatid disease that is seen mostly in Alaska, Canada, the Soviet Union, and central Europe. Environmental factors causing echinococcosis (Echinococcus multilocularis): Transmission of the fox tapeworm Echinococcus multilocularis, the causative agent of human alveolar echinococcosis, is known to depend on various environmental factors which are subject to human influence. Epidemiological data suggest that in most endemic regions landscape changes (Example: deforestation and agricultural practices) have led to more favourable conditions for the parasite's animal hosts, especially arvicolid rodents, thereby increasing the risk for parasite transmission and human disease. Examples are the conversion of forests or crop fields into meadows and pastures in Europe, China and North America, and overgrazing of natural grassland in central Asia. Other anthropogenic factors include interference with host population densities by wildlife disease control, changing hunting pressure and provision of new habitats, e.g. in urban areas. Domestic dogs may, under certain conditions, get involved in the otherwise largely wildlife-based transmission, and thereby greatly increase the infection pressure to humans. The introduction of neozootic host species may increase transmission, or even initiate the parasite's life-cycle in previously non-endemic regions. Lastly, the parasite itself may be accidentally introduced into non-endemic areas, if suitable host populations are present. Life Cycle: The definitive hosts for the adult cestode are carnivores, commonly the domestic dog for Echinococcus granulosus and the fox for Echinococcus multilocularis . The adult tapeworms which may number several thousands in the heavily infected dog intestine, shed both eggs and gravid proglotids, which can be found in the host's stool. Human and natural intermediate hosts become infected when they swallow these immediately infective eggs. In the duodenum the larvae or onchospheres are freed and using their hooklets, find their way through the intestinal mucosa into the lumen of blood vessels. They are then carried by the blood until they lodge in capillaries at almost any site. In 60% of cases, the larvae are retained in the sinusoids of the liver. The remainder pass through the hepatic circulation, and 20% are retained in the lung, the others gain access to the systemic circulation. The embryos of Echinococcus granulosus that survive develop into hydatid cysts containing numerous scolices provided with hooklets. These scolices represent the future head of the adult tapeworm. The cysts have an outer laminated, elastic layer and an inner germinal layer. They enlarge gradually for several months until they attain a diameter of 10 - 20 cm. Abundant clear fluid is contained within the cysts. The germinal layer develops numerous papillae, which becomes pedunculated vesicles (brood capsules) containing scolices. Cysts of echinococcosis occur more frequently in the liver or in the lung. Approximately 70% of primary echinococcal cysts are found in the liver and most of these are in the right lobe. Clinical presentation: It has been estimated that approximately 25% of people infected with Echinococcus go through life without any symptoms referable to the tapeworm. Symptoms may take a long time to develop for the disease progresses slowly. The cysts may become secondarily infected, suppurate, and produce the clinical picture of hepatic abscess. Some of the cysts may collapse and undergo fibrosis and in some cases there is calcification. The hydatid fluid, when liberated into the circulation, gives rise to pronounced eosinophilia. There may be allergic manifestations such as urticaria and angioneurotic edema. Diffuse implantaion in the peritoneal or pleural cavities may develop after rupture of subpleural and subperitoneal cysts. The disease is fatal in most untreated patients and in a significant percentage of those treated with surgery. Features: In Echinococcus multilocularis, the daughter cysts, which arise from the germinal membrane by budding, develop on the outside of the original (mother) cyst. This results in invasion of surrounding parenchyma by the new scolices, which are not contained by the laminated cuticular membrane. The pattern of growth resembles that of malignant neoplastic lesions. Diagnosis of the disease: The diagnosis of hepatic hydatid disease is suggested by the presence of an abdominal mass detected by palpation and confirmed by ultrasonography, liver scan or CT scans. The diagnosis must then be confirmed serologically. The various methods available include complement fixation, enzyme-linked immunosorbent assay (ELISA) or indirect hemagglutination. Immunodiagnosis: Accurate immunodiagnosis of the infection requires highly specific and sensitive antigens to be used in immunodiagnostic assays. The choice of an appropriate source of antigenic material is a crucial point in the improvement of the diagnostic features of tests, and must be based on the developmental stage of the parasite and the host. The most common antigenic sources used for the immunodiagnosis of echinococcal disease are hydatid cyst fluid, somatic extracts and excretory-secretory products from protoscoleces or adults of Echinococcus granulosus. Hydatid cyst fluid is the antigenic source of reference for immunodiagnosis of human hydatidosis, which is mainly based on the detection of antigens B and 5. Somatic extracts have been widely used in the serodiagnosis for Echinococcus granulosus infection in dogs and ruminant intermediate hosts, although in the last few years the detection of excretory-secretory products of the worm in faeces (coproantigens) have become the most reliable method for the detection of the parasite in the definitive host.
|
|
|
