

Custom Search
|

|
Infectious Disease Online
Pathology of Giardiasis
|
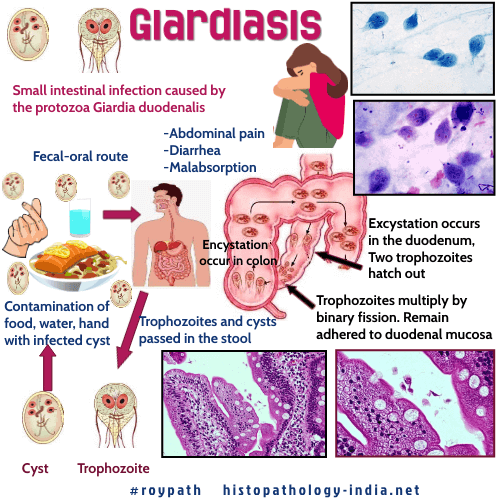
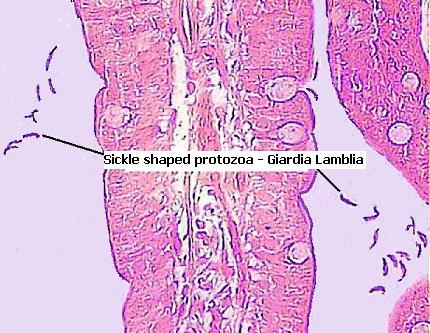
Giardiasis is a small intestinal infection caused by the protozoa Giardia duodenalis (also referred to as Giardia lamblia and Giardia intestinalis). Giardia duodenalis is a pear or sickle shaped, binucleate protozoa.
Giardia exists as infectious cysts in contaminated food and water
which spread by fecal-oral route and as trophozoites which multiply in
the intestinal lumen and cause disease.
Usually
asymptomatic. May present with epigastric or right upper quadrant pain
and persistent steatorrhoea. Increase in severity of the case correlate
with factors such as achlorhydria and low secretary IgA level (agammaglobulinemic
patients) How does it differ from Entamoeba histolytica? Giardia duodenalis trophozoites are pear-shaped,have two nuclei and are flagellated. Reside in the duodenum rather than colon. Adhere to the intestinal epithelial cell rather than invading the
epithelium, thus causing diarrhoea rather than dysentery. The
trophozoites adhere to the sugars on the intestinal epithelial cells via
parasite lectin which is activated when cleaved by proteases. Tight
contact is made between parasite and intestinal epithelial cell via
sucker-like disc. Histologic features: One or two duodenal punch biopsy specimens are adequate for diagnosis (site of colonization of organism may vary ). Diagnostic feature: Identification of sickle shaped organism attached to the surface or free within the mucus layer. Biopsy features range from normal to abnormal appearance of the intestinal mucosa. Mucosal changes are minimal in most cases. In some cases here may be clubbing of villus and decreased villus-crypt ratio. Crypt hyperplasia and focal epithelial damage may be noted. An increased mononuclear infiltrate may be present in the lamina propria. There may be increased intraepithelial lymphocytes. The brush border of the absorptive cells may be irregular. Sometimes villi may be absent and resemble atrophic stage of gluten-induced enteropathy. In case of immunodeficient patients, the histopathologist should look for plasma cells in the lamina propria. Nodular follicular hypertrophy of the mucosal lymphoid tissue is associated with common variable immunodeficiency. Crypt cell loss and apoptosis may be noted in HIV (human immunodeficiency virus) positive cases.
|
|
|
