
|

| Infectious Disease Online Pathology of Hookworm Infection (Ancylostomiasis)
|
|
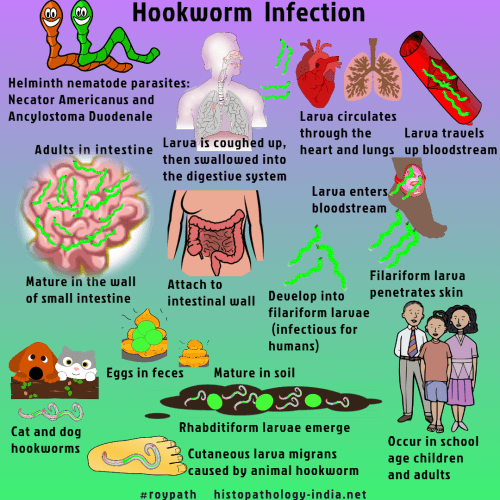
Hookworm
infection in humans is caused by an infection with the
helminth nematode parasites
Necator americanus and Ancylostoma duodenale. Mode of infection: Hookworms (Necator and Ancylostoma) are generally contracted by walking barefoot on soil contaminated by feces from infected animals or persons, or by swimming or wading in contaminated water. Hookworm infection is among the most important tropical diseases in humans. The greatest number of hookworm cases occur in Asia, followed by sub-Saharan Africa. Necator americanus is the most common hookworm worldwide, whereas Ancylostoma duodenale is more geographically restricted. In contrast to these major anthropophilic species, three species of zoonotic hookworm are minor causes of disease in humans. Ancylostoma ceylanicum infects dogs and cats and can also infect humans but is not considered an important pathogen. The dog hookworm Ancylostoma caninum causes human eosinophilic enteritis in northeastern Australia ,and Ancylostoma braziliense causes cutaneous larva migrans. Some of the highest rates of hookworm transmission occur in the world's coastal regions, where infective third-stage larvae can migrate freely in sandy soils and where temperatures and moisture are optimal for viability of larvae. In these areas, repeated exposure to third-stage larvae of Necator americanus or Ancylostoma duodenale results in a local pruritic, erythematous, papular rash known as "ground itch." [ Note: The three main soil-transmitted helminth infections, Ascariasis , Trichuriasis, and hookworm, are common clinical disorders in man. The gastrointestinal tract of a child living in poverty in a less developed country is likely to be parasitised with at least one, and in many cases all three soil-transmitted helminths, with resultant impairments in physical, intellectual, and cognitive development.]
The term "hookworm disease" refers primarily to the iron-deficiency anemia that results from moderate or heavy infection. In the passage through lungs, petecheal hemorrhages and areas of transient bronchopneumonia are produced.
Blood loss occurs when the worms use the well developed buccal capsule to attach themselves to the intestinal mucosa and submucosa (specially the duodenum and first portion of the jejunum) and contract the muscular esophagus to create negative pressure, which sucks a plug of tissue into their buccal capsules. There is damage of small areas of the mucosa producing punctate hemorrhages and at the same time they draw blood from the mucosa. Capillaries and arterioles are ruptured not only mechanically but also chemically, through the action of hydrolytic enzymes. To ensure blood flow, the adult hookworms release anticlotting agents. Some red cells undergo lysis, thereby releasing hemoglobin, which is digested by a cascade of hemoglobinases that line the gut of the parasite. The major clinical manifestations of hookworm disease are the consequences of chronic intestinal blood loss. Iron-deficiency anemia occurs and hypoalbuminemia develops when blood loss exceeds the intake and reserves of host iron and protein. Morphological changes in the small intestine in hookworm disease include villous atrophy and crypt hyperplasia. These changes and the malabsorptive state that is commonly present are probably unrelated to the infection. When severe anaemia occurs in young children, it retards growth as well as well as sexual and mental development. The presence of characteristic ova in stools, establishes the diagnosis. Serologic tests are available but play little role in clinical diagnosis.
|

![]()
Copyright © 2021 histopathology-india.net