

Custom Search
|

|
Infectious Disease Online Pathology of Lobomycosis
|
|
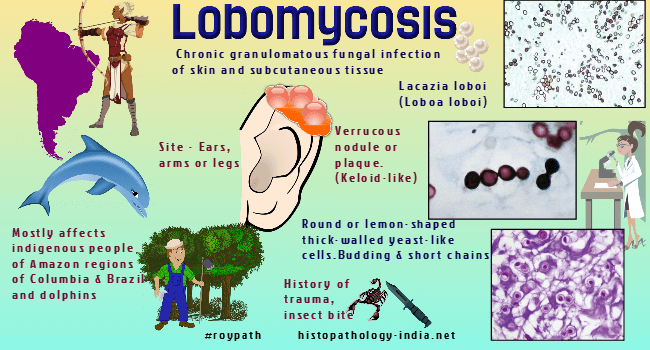
Syn: Lobo's disease, keloidal blastomycosis, lacaziosis Lobomycosis is a cutaneous mycosis characterized by a slowly developing variably sized cutaneous nodules after a traumatic event. Lacazia loboi ( Syn: Loboa loboi ) the etiologic agent, cannot be grown in culture. The lesions are composed of granulomatous inflammatory tissue containing numerous globose or subglobose to lemon-shaped, yeast-like fungal cells singly or in simple and branched chains. Natural infection occurs only in human and dolphins and produces locally enlarging cutaneous nodules that become verrucous.
Cases of lobomycosis involving two species of dolphins, namely, marine dolphins (Tursiops truncatus) and marine freshwater dolphins (Sotalia fluviatilis), have been reported. Clinical history: The onset of the disease is generally insidious. The increase in size or number of lesions is a slow process, progressing over a period of 40 to 50 years . The history often reveals the cause being a trauma, for example, an arthropod sting, a snake bite, a cut from an instrument, or a wound acquired while cutting vegetation. The causal agent of lobomycosis appears to be in aquatic environments, which probably plays an extremely significant part in its life cycle Geographic distribution: The human disease is endemic in the tropical zone of the New World and has been reported in central and western Brazil, Bolivia, Colombia, Costa Rica, Ecuador, Guyana, French Guiana, Mexico, Panama, Peru, Suriname, and Venezuela. Pathological features: The dermal nodules manifest as either smooth, verrucose, or ulcerated surfaces which can attain the size of a small cauliflower-like keloid. The yeast-like cells of Lacazia loboi are abundant in the dermis of the cutaneous nodules. These thick-walled cells, 6 to 12 micrometer in diameter, are remarkably uniform in size and shape. They reproduce by progressive budding in chains, three to eight cells in length, each of which resembles a “string of pearls”. Adjacent cells are connected to one another by tube-like isthmuses, and secondary budding may be observed. Nonbudding and single-budding cells are also present. The surrounding dermis contains a dispersed epitheloid and giant cell granulomatous inflammatory reaction. Diagnosis: Diagnosis is based on demonstrating the presence of globose, thick-walled yeast-like cells in lesion exudate or tissue sections. The organism multiplies by budding, and thus mother cells with single buds are often observed. These thick-walled, hyaline, spherical cells with chains of cells interconnected by tubular connections are the basis on which a diagnosis of lobomycosis rests. The thick-walled, budding hyaline cells with chains of conidia can be readily observed in tissue smears or exudates mounted in 10% KOH or in Calcofluor mounts. Treatment: The lesions are best treated by surgical excision.
|

|
|

![]()
Copyright © 2022 histopathology-india.net