

Custom Search
|

|
Infectious Disease Online Pathology of Measles (Rubeola)
|
|
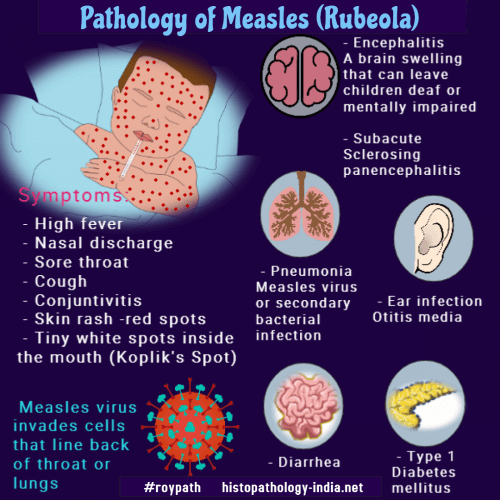
Measles is a highly infectious, systemic infection of
childhood, caused by measles virus.
Up to 6 months of age, infants are protected, due to antibodies from mothers, but thereafter are vulnerable. Measles vaccine has almost eliminated measles. Mode of infection: Humans are the only natural host. i) Infection is most commonly transmitted by inhalation of contaminated droplets. ii) May also be passed through the placenta. (Measles villitus : Image1 ; Image 2) Incubation period: About 14 days (10-21 days). Pathogenenesis: After infection, virus enters lymphoid tissue of tonsils, adenoids and lymphnodes with hyperplasia of reticuloendothelial system and then enters blood. It starts with symptoms of common cold and photophobia which develops by the 2nd day. Diagnostic "Koplik’s spots" are red irregular macules (1-3mm) with central white speck, appear on the buccal mucosa opposite 2nd molar tooth, around the opening of the parotid duct. In severe cases they can involve the entire mucous membrane of the mouth. After 3-4 days, "Koplik’s spots" disappear and blotchy, erythematous rash develops at the back of ears, which becomes maculopapular and rapidly spreads over face and down the neck, trunk and limbs. Nonproductive cough and fever increases. Rash clears with desquamation of epidermis and symptoms disappear within a few days. Serious and fatal complications are seen in immuno-compromised persons. Example: AIDS, child with malnutrition, neonates and elderly persons. Complications and sequela include otitis media, pneumonia (either measles virus or secondary bacterial pneumonia), measles encephalitis, subacute sclerosing panencephalitis, juvenile diabetes mellitus, and thrombocytopenic purpura. Microscopic features : Affected skin shows dilated epidermal vesicles, edema and a nonspecific, moderate inflammatory infiltrate of mononuclear and occasional neutrophils in the dermal capillary bed. Perivascular lymphocytic infiltrate may be present. The endothelial cells are swollen. Mitotic figures can be seen and vascular thrombosis with extravasation of erythrocytes may occur. Overlying epidermis shows hyperkeratosis and vacuolation of epidermal cells. Syncytial giant cells (Warthin-Finkeldey giant cell) are pathognomonic of measles. Giant cells contain both intracytoplasmic and intranuclear, eosinophilic inclusion bodies. These cells are found in "Koplik’s spots", lymphnodes Image Link1 ; Image link2 and other reticulo-endothelial organs. They are also found in lymphoid tissue of pharynx, bronchi, gastrointestinal tract including appendix. Giant cells disappear with appearance of circulating antibodies. Measles Giant Cell Pneumonia: It is usually seen in patients who fail to produce antibodies to virus. Example: AIDS. It occurs in children as massive pneumonia. Microscopic features: There is a florid mixed suppurative and interstitial pneumonia. Pulmonary parenchyma shows consolidation with large number of syncytial giant cells containing both intracytoplasmic and intranuclear, eosinophilic inclusion bodies. Similar giant cells are also seen in the tracheal gland epithelium. Respiratory epithelium may show squamous metaplasia. Immunohistochemistry identifies the virus infection. Visit: Subacute Sclerosing Panencephalitis
|
|
|
