

Custom Search
|


|
Dermpath-India Pathology of Nevoid Melanoma Dr Sampurna Roy MD 2022
|
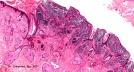
| Nevoid melanoma
is a rare form of nodular melanoma that may mimic benign melanocytic lesions. The lesions are called 'naevoid' because the cytological and architectural features resemble features of benign intradermal or compound melanocytic naevi. Recent studies have shown that there is a significant local recurrence and mortality rate in patients diagnosed with naevoid melanoma.
Immunohistochemistry: S100 protein and HMB45 are usually positive. The cells also express proliferating cell nuclear antigen (PCNA) and Ki67 (using MIB-1). HMB45 may be negative in some cases. Note: In Spitz naevus there is stratification of staining . In the base of the lesion cellular staining is less intense.
Similarities and differences between Nevoid melanoma and Spitz's Nevus: Nevoid Malignant Melanoma Large Cell Type: Similarities: (i) Cells tend to be large; (ii) Pagetoid cells may be present; (iii) Melanocytes are nested (iv) Cells may disperse at the base. Differences: Spitz's naevus : Mitoses present in dermis, but rarely at the base; cell size small at the base; Kamino bodies are common; HMB-45 patchy positivity, may be at base ; MIB-1 diminishes at base. Nevoid malignant melanoma (large cell type) : Mitoses present in dermis even at base; Cell size large at base ; Few Kamino bodies; HMB-45 positive at base; MIB-1 undiminished at base. Verrucous Nevoid Melanoma: Melanoma is characterized by epidermal hyperplasia , elongation of rete ridges and overlying hyperkeratosis. Clinically these lesions may be mistaken for seborrheic keratosis. (At low power some these lesions may resemble papillomatous benign intradermal naevi.) The tumour consists of small naevus like cells with no evidence of maturation with depth. The lesion may demonstrate atypical junctional component, asymmetric lateral growth pattern and area of regression.
|
|
|
