

Custom Search
|

|
Infectious Disease Online Pathology of Nocardiosis
|
|
Nocardiosis is
an infection of the lung that may spread to the brain and skin and
less commonly to the thyroid, liver, or other organs.
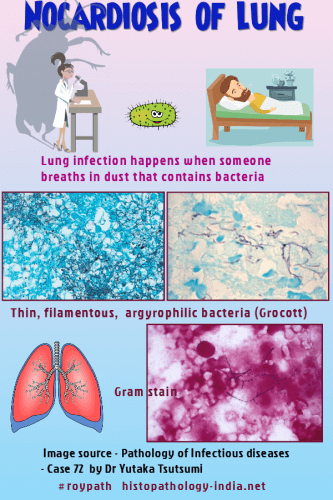
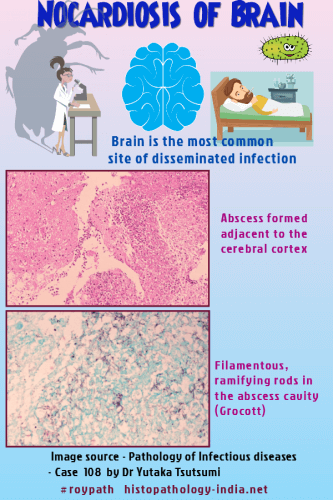
Causative organism: The causative organism is Nocardia asteroides, a gram-positive, aerobic, branching, filamentous bacillus that is weakly acid-fast and belongs to the order Actinomycetales. In about 85% of cases, infection is caused by Nocardia asteroides, and the remaining 15% are caused by Nocardia brasiliensis and Nocardia otitidiscaviarum (caviae). Distribution: Nocardia species inhabit the soil and have worldwide distribution. Mode of infection: Unlike actinomycosis, nocardiosis is an exogenous disease and infections are usually contracted by inhalation of nocardiae that live as saprophytes in nature. The disease is not contagious. Predisposing factors: Debility and immunosuppression predispose to infection. Well recognized conditions that predispose patients to nocardial infection include lymphoma, Hodgkin's disease, chronic granulomatous disease of childhood, and pulmonary alveolar proteinosis. Clinical presentation: Fever, weight loss, night sweats, and cough are usual. Invasion of the lung causes a bronchopneumonia, which may extend to become lobar. Direct extension to the pleura, trachea and heart and extension to the brain or skin through the circulation are recognized complications and carry grave prognosis. Pathological features:
Lungs: The gross appearance of lung depends on the duration and extent of infection. The lesions may be focal or diffuse and usually have necrotic centers surrounded by a perimeter of organizing pneumonia. Large cavitating abscesses may be present or there may be diffuse fibrinopurulent pneumonia similar to that caused by certain nonfilamentous bacteria. Fibrosis is usually minimal. Microscopically, the necrotic centers are rich in fibrin and degeneration neutrophils. The nocardia infiltrate the pulmonary tissue freely and are most easily seen after silver impregnation. A modified acid-fast stain demontrates weak and segmental staining. Central Nervous System: About 20% of patients with pulmonary nocardiosis have central nervous system involvement, usually in the form of cerebral abscesses. Meningitis, a rare complication, results from rupture of an intracerebral abscess or direct extension of nocardial osteomyelitis. Skin and subcutaneous lesion: Nocardiosis may also present as solitary or multiple subcutaneous lesions that are attributable either to traumatic implantation or to systemic infection. These localized lesions, with chains of nodules leading from a primary skin ulcer, can mimic those of cutaneous sporotrichosis. This entity is known as the sporotrichoid form of nocardiosis. Nocardia species: In systemic infections, the Nocardia species almost never form granules. Rather, these organisms occur as individual, gram-positive, beaded filaments, about 1 micrometer in width, that branch at approximately right angles. Special stains: The delicate filaments are not stained by hematoxylin and eosin, periodic acid-Schiff, or Gridley stains. However they are readily demontrated with Gomori methenamine-silver and tissue Gram stains. All three Nocardia species are often partially acid-fast in tissue sections when stained with modified acid-fast procedures using a weak decolorizing agent. Usually the agents of actinomycosis are not acid fast. Nocardia brasiliensis and Nocardia otitidiscaviarum (caviae) may cause pulmonary nocardiosis resembling that produced by Nocardia asteroides but more characteristically they may present as Mycetomas. They are inoculated into the skin and subcutaneous tissue at the time of penetrating trauma, grow slowly, and form nocardial grains. A pyogranulomatous reaction erupts through the skin to form draining sinuses. Nocardial mycetomas must be distinguished from the mycetomas caused by fungi and nonfilamentous bacteria. Sulphonamides are useful for treating all forms of the disease. Because of a strong tendency for relapse, prolonged therapy may be required. |
|
|

![]()
Copyright © 2021 histopathology-india.net