

Custom Search
|

|
Infectious Disease Online Pathology of Onchocerciasis (River Blindness)
|
|
The filarial nematode
that causes onchocerciasis is known as Onchocerca volvulus. Geographic distribution: The disease is seen in west and central Africa and in circumscribed areas of Mexico, Guatemala, Venezuela and Columbia and in parts of Yemen. Mode of transmission: Onchocerciasis is transmitted by small flies of the genus Simulium (gnat or black fly); These tiny flies ingest the microfilariae when they bite an infected person ; After undergoing several transformations in the body of the fly, the microfilariae finally develop into infective larvae ; The larvae are introduced into the skin of a person who is bitten by the fly ; The organisms travel freely along the dermis but appear only rarely in the blood or internal organs ; They have been identified in the lungs, liver, spleen, and kidneys. Clinical presentation: It is one of the leading causes of blindness in the developing world. Although onchocerciasis is also known as river blindness, it is not just a disease of the eyes, but rather a chronic multisystem disease. Clinically, onchocerciasis takes three forms : 1) Eye disease ; (2) Subcutaneous nodules; and (3) A pruritic hypopigmented or hyperpigmented papular dermatitis. Ocular Lesions: The most serious complication of the migratory phase of the microfilariae in onchocerciasis is the ocular involvement. Microfilariae may invade the eyeball. A prominent horizontal punctate keratitis produced by the reaction of the corneal tissue to microfilariae is the most common finding. The keratitis does not appreciably reduce the visual acuity of these patients. When microfilariae reach the vitreous humor and penetrate the ciliary body, visual impairment develops. Photophobia, lacrimation and finally blindness result. Secondary change of a degenerative type develop in the crystalline lens ; anterioe synechiae are formed after exudation of fibrin and leukocytes into the anterior chamber. The posterior chamber and optic nerve are also occasionally affected. The outcome of all these processes is total blindness with glaucoma and phthisis bulbi. For this reason the disease entity is commonly referred to as "river blindness".
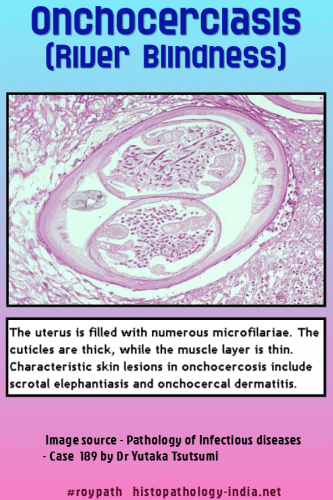
Cutaneous and Subcutaneous Lesions: The skin problems include troublesome itching , acute and chronic papular onchodermatitis, depigmentation and lichenified onchodermatitis . Migration of the microfilariae from the onchocercotic nodules to the adjacent dermis produce irritation of the skin. Small hemorrhages and an inflammatory reaction are seen microscopically. Edema and thickening of the skin and subcutaneous tissue develop after several months. Itching in some cases may be severe. When the onchodermatosis is conspicuous in the facial region, leionine facies may develop. Leopard skin shows foci of epidermal atrophy and elastic fiber breakdown alternating with areas of hyperkeratosis , hyperpigmentation with pigment incontinence, dermal atrophy, and fibrosis. Other typical varieties of onchocercal skin diseases include hanging groin, lymphoedema and marked lymphadenopathy. Lymphadenitis and rarely genital elephantiasis may develop in African patients. Obstructive lymphadenitis involving femoral and inguinal lymphn nodes is believed to be the result of inflammation and fibrosis caused by immune-complex deposition. Cutaneous nodules: The larvae mature in the dermis and produce solitary or multiple cutaneous nodules called onchocercomas which are characterisitic of this disease. In the African variant of the disease: The nodules are limited to the skin over the pelvic bones and lower limbs. In the Central American variant: The nodules are usually located in the scalp and the skin of the face and neck. There is however considerable overlapping between these two variants of the disease. The nodules represent an inflammatory reaction to the adult worms. Adult worms in small clefts are present in the onchocercomas usually in the proportion of two or more males to each female. The worms may be alive or dead. The inflammatory reaction is greater around dead worms. Histiocytic proliferation and foreign-body giant cell reaction are seen around many of the dead parasites. There is an accompanying prominent infiltration of polymorphonuclear leukocytes. Some chronic inflammatory cells and eosinophils may be present. There may be dense fibrosis so that nodule is replaced by dense collagenous fibroconnective tissue. The nodule may erode adjacent bone. Variable numbers of microfilariae are present in the surrounding areas. Investigation: - Detailed clinical history : Patients living or travelling to endemic areas are at risk. - Identification of the microfilariae in skin biopsy samples (skin snips) and demonstration of adult worm in sections from subcutaneous nodules. - Examination of blood and body fluid. - Slit-lamp examination: May reveal microfilariae in the anterior chamber. - Immunodiagnosis: Serologic methods of complement fixation and enzyme immunoassay are also available. - Mazzotti Test: Reaction to oral diethylcarbamazine (DEC) which kills microfilariae and produces allergic erythema and pruritus. - Nodulectomy removes adult worms in palpable nodules but misses deeper worms. - River blindness is being dramatically reduced in West Africa by the aggressive distribution of the antihelminth drug ivermectin.
|
|
|

![]()
Copyright © 2021 histopathology-india.net