
|

|
Infectious Disease Online Pathology of Talaromycosis (Penicilliosis) - Talaromyces Marneffei Infection
Talaromyces marneffei is a dimorphic fungus in the genus of Penicillium.Talaromyces marneffei infection (Talaromycosis) is endemic among HIV-positive patients in many areas in Southeast Asia. |
|
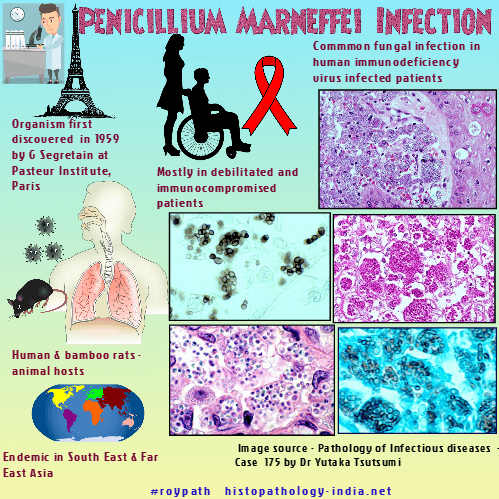
The first report of human infection due to Talaromyces marneffei (previously known as Penicillium marneffei)was reported by G. Segretain at the Pasteur Institute in Paris in 1959. He accidentally pricked his finger with a needle containing the yeast cells of T.marneffei. Talaromycosis is a disseminated and progressive infection and is the third most common opportunistic fungal infection in human immunodeficiency virus (HIV)-infected patients in certain parts of Southeast Asia. Talaromyces marneffei infection is endemic in Southeast Asia and Far East Asia, particularly in the southern part of China. Cases have been reported from both Eastern and Western countries. Of the more than 150 recognized species of Penicillium, only Talaromyces marneffei is known to be dimorphic and to cause invasive infection. Prior to the epidemic of human immunodeficiency virus (HIV), Talaromycosis was a rare event. The incidence of this fungal infection has increased markedly during the past few years, paralleling the incidence of HIV infection. Human and bamboo rats are the only known animal hosts of Talaromyces marneffei. Mode of infection: Most human infections probably have a pulmonary inception after inhalation of airborne infectious conidia of Talaromyces marneffei produced in the environment. Persons who are debilitated or immunocompromised appear to be at increased risk of infection.
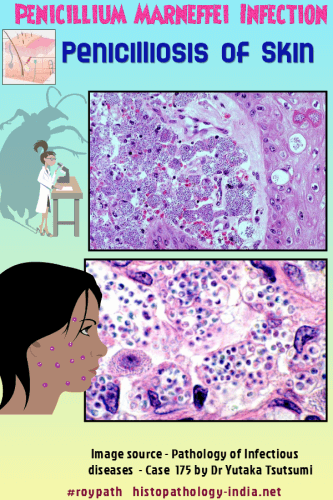
Clinical presentation: Patients with disseminated Talaromyces marneffei often present with chronic productive cough, mucoid sputum, chest pain, generalized lymphadenopathy , hepato-splenomegaly, draining skin ulcers, subcutaneous abscesses, osteolytic lesions, anemia, leukocytosis and a history of weight loss and prolonged intermittent fever. The skin lesions are most commonly papules with central necrotic umbilication. Course of the disease : The course of the disease can range from 2 months to 3 years or more. Organs involved: Organs most frequently involved include the lungs, liver, intestine, lymph nodes, tonsils, skin, bone marrow, kidneys, and spleen. Pathological Features: The host response in Talaromyces marneffei is similar to that seen in histoplasmosis , where numerous small yeast-like cells proliferate within and distend histiocytes. Visit: Histoplasmosis Slowly evolving pulmonary abscesses and granulomas can lead to fibrosis and cavitation, but calcification has not been reported. In histologic sections, the cells of Talaromyces marneffei are spherical to oval,2.5 to 5 micrometer in diameter, and resemble those of Histoplasma capsulatum. However, unlike histoplasma and other invasive yeast-like fungi, Talaromyces marneffei does not bud. Reproduction is by fission (schizogony) with the formation of a single transverse septum that stains more intensely with the special stains for fungi and is wider than the external wall. Short hyphal forms and elongated, curved sausage-like forms with rounded ends and one or more septa are also occasionally produced, especially in the necrotic and cavitary lesions. Diagnosis: A definitive diagnosis of Talaromyces marneffei infection can be made by demonstration of typical yeast-like cells in clinical specimens and by microbiologic culture an standard mycologic media. Treatment: The mycosis must be aggressively treated with amphotericin B, 5-fluorocytosine, or keratoconazole. Because relapse is common, antifungals should be given for several months. |
|
|

![]()
Copyright © 2022 histopathology-india.net