

Custom Search
|

|
Infectious Disease Online Pathology of Tularemia
|
|
Tularemia is an acute, febrile, granulomatous, zoonotic disease caused by Francisella tularensis. Rabbits and rodents are the most important reservoirs, but many other wild and domestic animals are infected. Humans become infected through broken skin or intact mucosa by handling infected animals and carcasses ; by ingesting contaminated food and water ; by inhaling bacteria ; or by being bitten by infected insects, including ticks, deer flies, and mosquitoes. Human-to-human transmission has not been reported. Bioterror attacks and other world events have focused the medical community's attention on agents that might be used in biological warfare. One of these potential biological weapons is Francisella tularensis, that is one of the most infectious bacteria known. Francisella tularensis can cause severe, even fatal, systemic tularemia. As a weapon of terrorism, the bacterium would likely be disseminated as an aerosol and contracted by inhalation. Francisella tularensis is a small (0.2 by 0.5 micrometer), aerobic, gram-negative bacillus that is not motile, encapsulated, or spore-forming. It does not grow in the standard bacteriologic media, but will grow slowly on media enriched with cystine or cysteine. Two types of Francisella tularensis are identified. Type A : In United States only where it causes 90% of tularemia). It is highly virulent and is usually tick-borne and rabbit associated. The mortality from untreated Type A tularemia ranges from 5% for ulceroglandular tularemia to 30% for the typhoidal and pneumonic forms. Type B : It is less virulent and has a worldwide distributation. It occurs in goats and may be transmitted to humans by mosquitos or ticks, or by water contaminated by infected rodents, such as beavers and muskrats. The mortality caused by Type B is less than 1%, even if the disease is left untreated. In humans, tularemia is classified into six major syndromes: ulceroglandular (the most common form), glandular, typhoidal, oculoglandular, oropharyngeal, and pneumonic. Pneumonia may complicate any one of the types. The incubation period ranges from 1 to 20 days, depending on the dose and route of transmission, with a mean of 3 to 4 days. The duration of illness is 1 week to 3 months, but may be shortened by prompt treatment. The most common form of tularemia, ulceroglandular, begins as a tender erythematous papule at the site of inoculation, usually on a limb. This develops into a pustule, which ulcerates. The regional lymph nodes become large and tender and may suppurate and drain through sinus tracts. In some patients an erythematous, maculopapular rash, thought to represent delayed hypersensitivity, may develop. The initial bacteremia is followed in a week by generalized lymphadenopathy and splenomegaly.
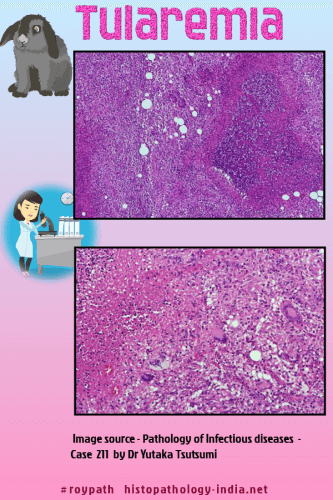
Symptoms include fever, headache, myalgia, and occasionally prostration. Some patients develop meningitis, endocarditis, pericarditis, or osteomyelitis. The most serious infections are complicated by a secondary pneumonia and endotoxic shock, in which case the prognosis is grave. In oculoglandular tularemia the primary lesion is a papule in the conjunctiva, which becomes a pustule and ulcerates. This is accompanied by lymphadenopathy of the head and neck. Severe ulceration may penetrate the sclera entering the eye and infect the optic nerve, causing blindness. In glandular tularemia generalized lymphadenopathy is the first manifeatation. A diagnosis of the typhoidal form is made when fever, hepato-splenomagaly, and toxemia, resembling salmonella sepsis, are presenting features. Diagnostic antibody titers usually appear within 2 weeks of infection. The initial skin lesion in tularemia is a pyogenic ulcer with purulent exudates. Later, disseminated lesions undergo central necrosis and are surrounded by a perimeter of granulomatous reaction resembling lesions of tuberculosis. The lymphnodes become large and firm from hyperemia and large numbers of histiocytes in the subcapsular and peritrabecular sinusoids. Later they soften as area of stellate necrosis and suppuration develop. By contrast, the enlarged spleen shows only congestion, nonspecific inflammatory cell infiltrates, and lymphoreticular hyperplasia. The lesions in the lung resemble those of primary tuberculosis. Image by Dr Yale Rosen On rare occasions bacilli may be identified in histiocytes. |
|
|
