Custom Search
|

|
Infectious Disease Online Pathology of Primary Amebic Meningoencephalitis (PAM) caused by Naegleria Fowleri, (Naegleriasis)
|
|
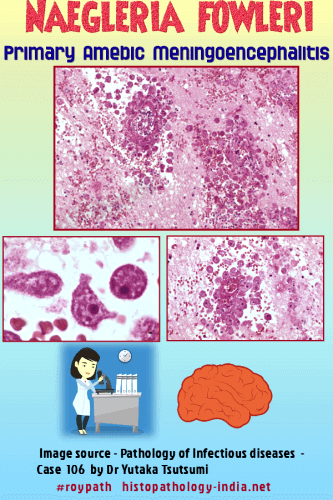
Primary amebic meningoencephalitis (PAM), caused by Naegleria
fowleri , is characterized by acute suppurative inflammation of the
brain and meninges.
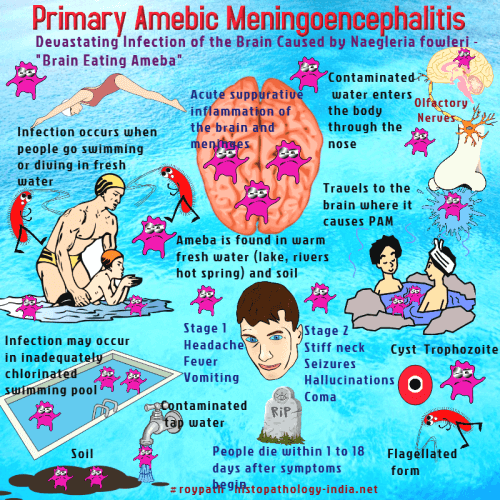
Naegleria fowleri is a nonparasitic, free-living soil ameba that causes rhinitis when introduced into the nasal cavity. The amebae may subsequently invade the olfactory nerves, migrate through the cribriform plate, and proliferate in the meninges and brain.
The infections are fulminating and uniformly fatal. The disease has been recognized in many parts of the world including the United States, Europe, Australia, New Zealand, South America, and Africa. It has been diagnosed principally on histologic evidence, with only a few cases confirmed by cultures. Almost all patients give a history swimming in freshwater lakes or pools shortly before the onset of symptoms. In tissue sections, trophozoites of Naegleria measure from 8 to 15 micro meter across. The cytoplasm is not distinctive, but the nuclei are sharply outlined and deep stained with hematoxylin. Some amebae have perinuclear vacuoles that tend to obscure the nuclear margin. Cysts of the Naegleria have not been seen in tissue sections.
Clinically, acute and fulminating rhinitis and meningoencephalitis lead to death, usually within 1 to 2 weeks. Most victims have been in their teens or younger. The cerebrospinal fluid contains numerous neutrophils, blood, and amebae. Grossly, the brain is swollen and soft, with vascular congestion and a thin purulent exudates on the meningeal surface, most prominent over the lateral and basal areas. There is massive destruction of the brain by amebae, which invade the brain along the Virchow-Robin spaces. Thrombosis and destruction of blood vessels are associated with extensive hemorrhage in the affected areas. The olfactory tract and bulbs are enveloped and destroyed, and there is an exudate between the bulb and the inferior surface of the temporal lobe.
During life, diagnosis is made by finding organisms in the cerebral spinal fluid or in biopsy specimens. The fluid may be placed directly in the counting chamber, where motile amebae are seen.
|