

Custom Search
|

|
Infectious Disease Online Pathology of Angiostrongyliasis
|
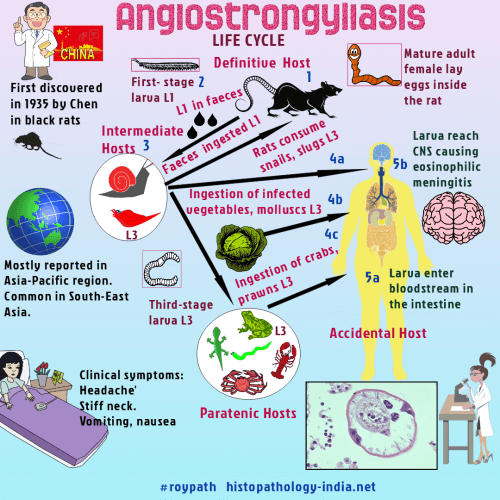
Angiostrongyliasis is infection with Angiostrongylus cantonensis (cerebral) or Angiostrongylus costaricensis (abdominal). Both are parasites of rats that accidentally infect humans.Angiostrongylus cantonensis (the rat lungworm) was first discovered in 1935 by Chen in black rats (Rattus rattus), in Canton, China.Angiostrongylus cantonensis is the most common cause of eosinophilic meningitis.The rodent is the definitive host while infected molluscs, snails and crabs act as the intermediate hosts.Humans are infected by the 3rd stage larvae, either by eating undercooked intermediate hosts or by consuming vegetables.It is a delicate nematode reported in Asia Pacific region most commonly in South-east Asia and has been reported from Taiwan, Thailand, Indonesia, Vietnam and Sri Lanka.The larvae migrate to the gray matter of the brain, where they molt before ultimately lodging in a pulmonary artery.After maturation, the worms lay eggs in the lung that hatch in situ.Larvae are coughed up, swallowed, and passed in the faeces.The life cycle is completed when larvae infect snails, which in turn are eaten by humans.Migrating infective larvae or young adult worms die in and around blood vessels and arteries in the brain and provoke an eosinophilic meningoencephalitis, with a low mortality (less than 1%).The diagnosis is based on the demonstration of A.cantonensis in cerebrospinal fluid.A. costaricensis, is found exclusively in Central America, infects the mesenteric veins of rats near the caecum, where it deposits eggs. After hatching, larvae migrate to the faecal stream, pass with the faeces, and infect snails or slugs. Infective larvae emerge from the snails or slugs on the slime trail. Humans become infected by eating material contaminated with the slime trail. Worms reach maturity in the human host and produce viable progeny. Large nodules composed of scar tissue, eggs, and larvae cause lower right quadrant pain. Surgical excision of the nodules, together with the appendix, relieves the symptoms. Eosinophils in the cerebral spinal fluid suggest the diagnosis. Simple analgesia is sufficient for mild cases. Treatment of those with severe symptoms remains controversial. Glucocorticoids, lumbar puncture to reduce intercranial pressure and antihelminthic agents have been used.
|
|
|
