

Custom Search
|

|
Infectious Disease Online Pathology of Dirofilariasis
|
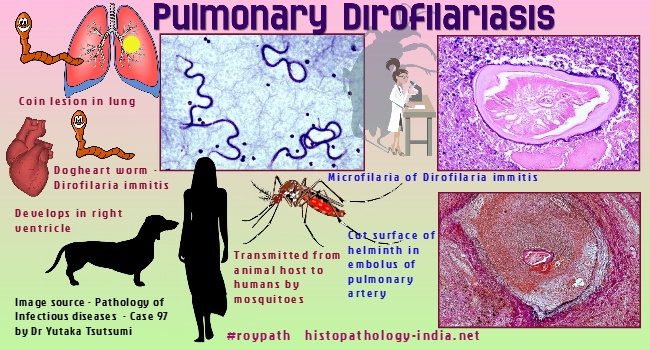
Pulmonary Dirofilariasis:The filarial nematode Dirofilaria immitis, a common parasite of dogs, cats and other mammals, is transmitted by mosquitoes.In humans the infective stage usually does not reach maturity, but is swept by the venous circulation into the lung, where it obstructs a pulmonary arteriole and causes a subpleural infarct, which resolves as a granuloma. Originally reported from Japan and Australia, pulmonary dirofilariasis is most common in the southern and eastern United States. Most of these lesions are silent and are discovered as spherical, 1cm to 3cm, subpleural "coin lesions" during radiologic examination of the chest. Microscopically, a central area of coagulation necrosis is surrounded by a zone of granulomatous reaction. The coiled immature and degenerating Dirofilaria immitis is located in an arteriole in the central zone of necrosis. Lesion may be resected using video-assisted thoracic surgery (VATS) which appear to be the best method for diagnosing pulmonary dirofilariasis. Subcutaneous Dirofilariasis:
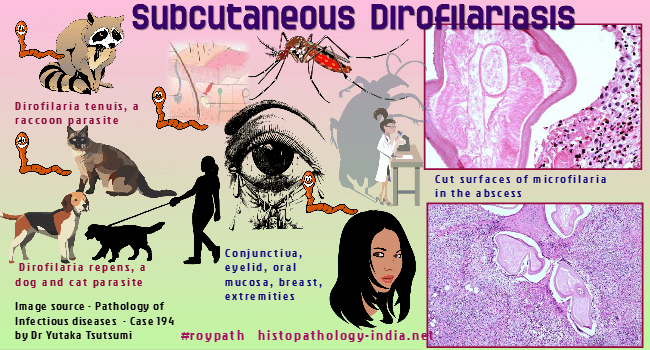
Dirofilaria tenuis, a subcutaneous parasite of the racoon, and Dirofilaria repens, a subcutaneous parasite of dogs and cats in Europe, Africa, and Asia, cause subcutaneous dirofilariasis in humans. Each of these species is probably transmitted to humans by mosquitoes. Before reaching maturity, the infective stage of the worm degenerates and provokes an abscess, usually surrounded by a granulomatous perimeter. The most common site is the subcutaneous tissue of the trunk, but the conjunctiva, eyelid, scrotum, and breast can also be affected. Clinically, a subcutaneous tender nodule gradually enlarges for several weeks. Microscopically, a central abscess contains a single coiled worm. Older lesions are granulomatous. The diagnosis is made by identifying the worm in a biopsy. |
|
|

![]()
Copyright © 2022 histopathology-india.net