| Kikuchi-Fujimoto disease (KFD), also called histiocytic necrotizing
lymphadenitis,
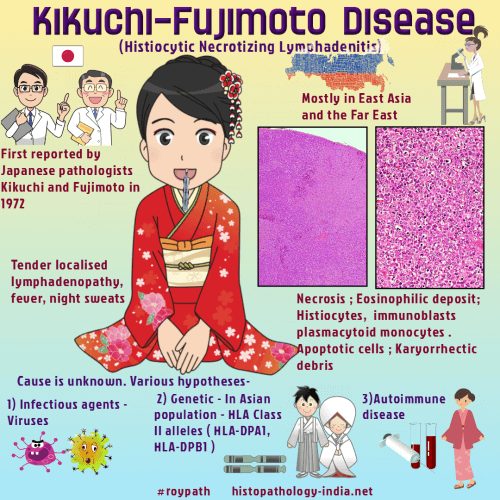
was initially reported in 1972 by Japanese pathologists Kikuchi and
Fujimoto.
They described the
disease as "lymphadenitis with focal proliferation of reticular cells
accompanied by numerous histiocytes and extensive nuclear debris."
It
is a rare, benign, and self-limited syndrome of unknown etiology
characterized by tender localized lymphadenopathy, constitutional
symptoms such as fever and night sweats.
Kikuchi-Fujimoto disease occurs in patients during third and fourth
decade of life and is usually more common in women than in men.
The
disease is more prevalent in Asian populations may be related to the
presence of certain HLA alleles such as HLA class II alleles,
HLA-DPA1 and
HLA-DPB1, which are more prevalent
in Asian patients. Although more prevalent in Asia,
some cases have been
reported in other continents also. The common laboratory abnormalities are leukopenia, usually
neutropenia, anemia, thrombocytopenia , elevated C-reactive protein
and erythrocyte sedimentation rate, impaired liver function and
atypical lymphocytes on peripheral blood smear.
Diagnosis is confirmed
histopathologically.
In Kikuchi-Fujimoto
disease,the most common histologic finding is lymph node showing
geographic necrosis with foci of apoptotic cells with abundant
karyorrhectic fragments surrounded by histiocytes. Characteristically,
neutrophils and eosinophils are absent.
Etiology of Kikuchi-Fujimoto disease has remained unknown, although
various infectious agents have been suspected like
Yersinia enterocolitica,
Brucella,
Bartonella henselae,
Entamoeba histolytica,
Toxoplasma gondii. and viruses
such as Epstein-Barr virus, herpes virus, cytomegalovirus, parvovirus,
paramyxovirus, parainfluenza virus, Rubella, hepatitis-B, human
immunodeficiency virus (HIV), human T-lymphotropic virus type-1
(HTLV-1), and the Dengue virus.
Because of the clinical and pathological correlation between
Kikuchi-Fujimoto disease and Systemic Lupus Erythematosus, some
authors have postulated that KFD may be a clinical feature or an
incomplete phase of lupus lymphadenitis. Clinical and histological differential diagnoses of Kikuchi-Fujimoto
disease include non-Hodgkin lymphomas and other lymphoid malignancies, lymphadenopathies associated with connective disorders such as SLE,
rheumatoid arthritis, and Still’s disease and bacterial or viral
infections such as cat scratch disease, infectious mononucleosis,
herpes simplex, HIV, toxoplasmosis, tuberculosis, and atypical
mycobacterial lymphadenitis.
|