|
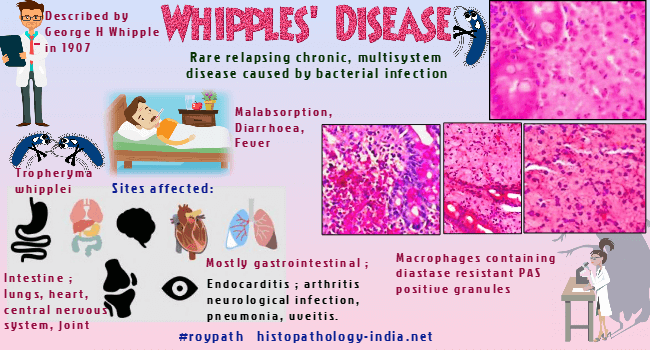
Whipple's disease is a rare chronic, relapsing, and multisystem disease
caused by bacterial infection.
It was first described
by George H. Whipple in 1907 and in 1949, the typical histological
picture of the intestinal mucosa was described displaying foamy
macrophages with cytoplasmatic periodic acid-Schiff (PAS) reactivity.
The etiology was
further clarified in 1961 by detecting bacteria by electron
microscopy.
Causative organism:
Gram-positive organism named Tropheryma whipplei. The name of this
bacterium—Tropheryma whipplei—is derived from Greek "trophe" (nourishment
and food) and "eryma" (fence and barrier).
Age: Patients in fourth
and fifth decade of life.
Clinical
presentation:
May present with a variety of rather nonspecific symptoms like malabsorption, diarrhoea, weight loss
and fever. The patient may also present with lymphadenopathy, hyperpigmentation and polyarthritis.
Sites
affected:
Intestine, central nervous system, joints, lymphnodes, lungs and heart.
Gross features:
The
affected bowel is usually edematous with yellow plaque-like lesions and
villiferous mucosa.
Affected lymph nodes appear yellow with a spongy cut
surface.
Other affected organs, such as lungs and heart, may show plaques
and edema.
Microscopic
features:
Small intestinal mucosa filled with distended macrophages in the lamina propria.
The macrophages contain
diastase resistant PAS positive granules.
Villi may be distorted.
Inflammation is usually absent.
Mesenteric lymphnodes may be involved and may show lymphatic dilatation
indicating lymphatic obstruction.
Microscopic
findings in the CNS include PAS-positive intracellular and extracellular
organisms surrounded by reactive astrocytes.
The organisms may also
violate the subarachnoid spaces and lead to the death of neurons,
vacuolization, and demyelination.
Diagnosis:
The diagnosis is usually established by small intestinal biopsy, which
shows the pathognomonic periodic acid Schiff-positive infiltrates in the
lamina propria.
The rod shaped
bacilli may be demonstrated by electron microscopy.
Polymerase chain
reaction is now available to aid in the diagnosis of WD, and this organism
has been identified by polymerase chain reaction in many body fluids,
including cerebrospinal fluid, aqueous humor, and synovial fluid.
Detection in
cerebrospinal fluid and peripheral blood is less consistent than in
tissue.
Differential
diagnosis: Includes AIDS
enteropathy caused by Mycobacterium avium intracellulare
(Ziehl-Neelsen
staining
positive).
Patients respond well to antibiotic therapy, but relapses occur.
|