

Custom Search
|


|
Dermpath-India Pathology of Fibroma of Tendon Sheath
|
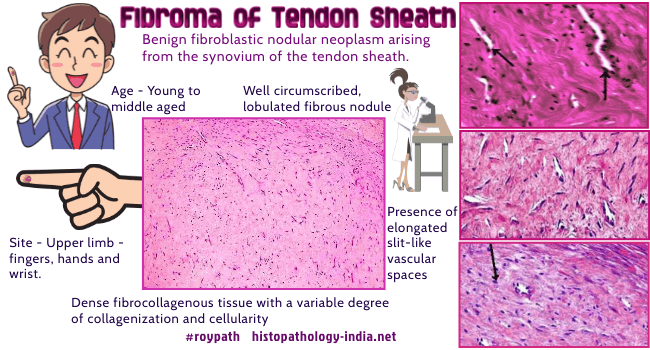
Benign fibroblastic nodular neoplasm that arises from the synovium of the tendon sheath that occurs mostly around small joints such as the fingers, hands, and wrist. Fibroma of tendon sheath was first described by Geschickter et al. in 1949. Age: Young to middle aged individuals. Sex:
It is more common in males
than females, with a ratio of 3 to 1. They are firm and rubbery and on section have a grayish-white appearance. Microscopic features: The lesions consist of a dense fibrocollagenous tissue with a variable degree of collagenization and cellularity, the peripheral zone often being most cellular and containing slit-like vascular spaces. In some cases there may be complete hyalinization. Mitotic activity depends on the cellularity of the lesion. Other features: Presence of inflammatory cells and myxoid stroma in some cases. Rare presence of giant cells or foamy cells. Immunohistochemistry: Vimentin - Positive ; muscle-specific actin and smooth muscle actin - Positive. Desmin - Negative ; Factor XIIIa- Positive ; CD34- Positive ; CD68 (+/- ). Cytogenetics: Transclocation 2;11 has been found in one case. Electron-microscopy: Two main cell types were identified: Myofibroblasts and fibroblasts, the former dominating in cellular areas, the latter dominating in collagenized areas.
Differential diagnosis: Giant cell tumour of tendon sheath (localised nodular tenosynovitis) ; Circumscribed fibromatosis ; Nodular fasciitis; Neurofibroma ; Leiomyoma ; Scar tissue ; Benign fibrous histiocytoma ; Comparison with Giant cell tumour of tendon sheath: This lesion is more common than fibroma of tendon sheath. Histologically, the two tumours have separate and distinct histologic features. Fibroma of the tendon sheath is hypocellular, with slit-like vascular channels within a dense collagen matrix , whereas giant cell tumor of the tendon sheath is much more cellular and contains multiple multinucleated giant cells, foamy histiocytes, and hemosiderin. All cases are treated effectively by local excision or reexcision of the growth.
|
|
|
