

Custom Search
|


|
Pathology of Granuloma Annulare Dr Sampurna Roy MD
|
|
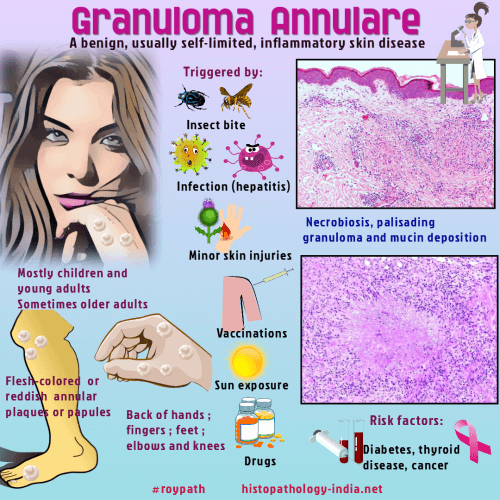
Granuloma annulare (GA) is a benign
inflammatory, self-limiting granulomatous dermatoses that is seen in
both adults and children. Females are more commonly affected than males. The lesions may involve skin and/or subcutaneous tissue. The etiology of granuloma annulare is unknown. The lesions could be related to insect bites, sun exposure, viral infections, diabetes, thyroiditis, immunoglobulin-mediated vasculitis, and certain medications such as antibiotics, antiinflammatory agents and oral contraceptives. Cases have also been reported in patients with AIDS, sarcoidosis, hepatitis C infection, Hodgkin's and non Hodgkin's lymphoma, metastatic adenocarcinoma and granulomatous mycosis fungoides. Clinical variants:
(1) Localized - Children
and young adults. Papules and annular or arciform
plaques. (2) Generalized - Middle aged and elderly patients. Multiple macules,
papules or nodules. (3) Perforating - Middle aged
and elderly females. Papules and annular
plaques. Scaling and crusting with central umbilication may be present.
(4) Subcutaneous or deep form - Children
and young adults. Solitary or
multiple nodules (a few millimeters to several centimeters in size).
Histological patterns in Granuloma Annulare: 1. Necrobiotic granuloma 2. Interstitial or 'incomplete' form - Most common 3. Granuloma of sarcoidal or tuberculoid type - Rare
Features of interstitial or 'incomplete' form of Granuloma Annulare: - Should be assessed under low power. - "Busy dermis" - increased number of inflammatory cells in the dermis separated by connective tissue mucin. - Infiltrate composed of lymphocytes and histiocytes. - Inflammatory cells are noted around blood vessels and between collagen bundles. - No well-defined areas of necrobiosis Differential diagnosis: (1) Interstitial Granulomatous Drug Reaction: Eosinophils (+) , lichenoid changes at dermoepidermal junction, true necrobiosis is rarely noted . (2) Interstitial Granulomatous Dermatitis: Neutrophils, neutrophil fragments, histiocytes, lymphocytes and eosinophils are present,palisades of histiocytes around basophilic collagen fibres. Changes may involve the full thickness of the dermis. Features of Subcutaneous Granuloma Annulare- (Pseudorheumatoid Nodule): - Located in the deep dermis, subcutis and rarely deep soft tissue. - Area of necrobiosis is larger than the superficial type. - Granulation tissue and lymphoid aggregates may be present near palisaded granuloma. - Eosinophils are more common in this variant. Differential diagnosis: Rheumatoid Nodule : Rheumatoid nodule and subcutaneous granuloma annulare. A comparative histologic study. Necrobiotic foci contain abundant fibrin. Degenerated bundles of collagen (+/-). Palisade of elongated histiocytes. Features of disseminated form of granuloma annulare: - Poorly formed granulomatous foci in the papillary dermis. - Necrobiosis is not prominent. Differential diagnosis: Lichen Nitidus : Claw-like acanthotic elongation of rete-ridges at the periphery of the lesion is absent in Granuloma annulare. Non-necrobiotic sarcoidal or tuberculoid type of Granuloma annulare: Rare variant. Dermal mucin and eosinophils help in distinguishing this lesion from sarcoidosis. Perforating Granuloma Annulare: Epidermal perforation connected to the underlying necrobiotic granuloma.
|
|
|
