

Custom Search
|

|
Infectious Disease Online Pathology of Haemophilus Influenzae Infection
|
|
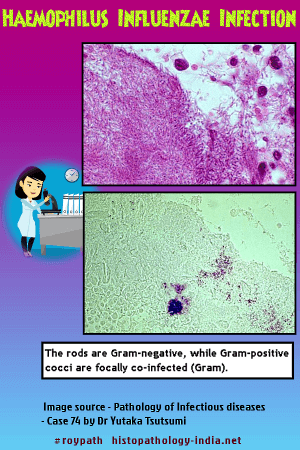
Haemophilus influenza is a gram-negative, pleomorphic, aerobic bacillus that is non-motile and does not form spores. It is a strict parasite of humans, and causes pneumonia, meningitis, epiglottitis, pericarditis, bacteremia, cellulitis, pyarthrosis (acute suppurative arthritis) , and "pink eye" - an acute purulent conjunctivitis. The presence or absence of a polysaccharide capsule determines the morphology of its colonies and its pathogenicity. Encapsulated bacteria secrete a capsular polymer that makes the colony appear umbilicated. Of six dissimilar antigens in the capsule, type B causes more than 90% of human infections and is the most common cause of bacterial meningitis. Haemophilus influenzae is recovered from 80% of healthy adults and is encountered worldwide. By 5 years of age, all children have Haemophilus influenzae in their nasopharynx, and 1 in 200 children will at some time have a systemic infection caused by type B. Some children who become infected before 18 months fail to develop adequate antibodies and may contract a second systemic infection with Haemophilus influenzae. Children under 2 years of age in day care centers or who are in families with an ill patient are at greater risk.
Meningitis caused by Haemophilus influenzae usually follows otitis, sinusitis, pneumonia or impaired immunity. An early symptom is pain when the child sits up or is diapered. Upper respiratory symptoms, fever, vomiting, irritability,and lethargy accompany the meningitis, and 5% to 10% die within 48 hours. Neurologic deficits are permanent in one-third of those who survive. Bacteria, neutrophils, and fibrin form an exudate in the leptomeninges. The exudate extends from the basal portion of the subarachnoid space into the brain along the vessels. The typical gram-negative coccobacilli are in neutrophils in the exudates around the meningeal blood vessels.
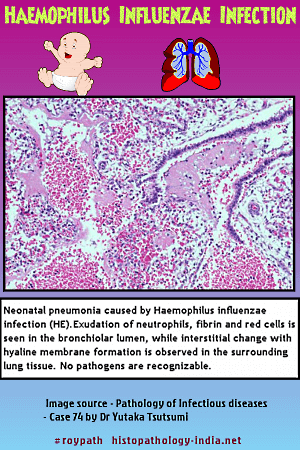
Infection of lung by Haemophilus influenzae produces fever, cough, purulent sputum, dyspnea, and either bronchopneumonia or lobar Pneumonia. The pneumonia usually complicates chronic lung disease and in half the patients follows a viral infection of the respiratory tract. The alveoli are filled with neutrophils, macrophages containing bacilli, and fibrin. The bronchial epithelium is necrotic and replaced by macrophages. Bacilli are in macrophages and short and long filamentous bacilli are packed together in extracellular foci. Empyema may form and display a similar inflammatory reaction. Part of the pathogenicity of Haemophilus influenzae may be due to an extracellular toxin that arrests the action of cilia. The onset of epiglottitis is sudden. Fever, dysphagia, accumulation of oropharyngeal secretions, tachypnea and retraction precede obstruction of airways. The epiglottis is swollen by edema, neutrophils, and macrophages.
The infection may descend past the larynx into the trachea and bronchi, plugging the small airways with thick exudates. Bacteremia may seed large weight-bearing joints, leading to pyarthrosis. There is fever, heat, erythema, swelling, pain on movement, and decreased movement. The diagnosis is made by culturing Haemophilus influenzae from the joint fluid. Needle aspirates of exudates from empyema and lung, pericardium, joint and blood or cerebral spinal fluid may be cultured for specific diagnosis. Chloramphenicol remains the drug of choice in meningitis.
|
|
|

![]()
Copyright © 2022 histopathology-india.net