Custom Search
|
|
Custom Search
|
|
Infectious Disease Online Pathology of Impetigo
|
|
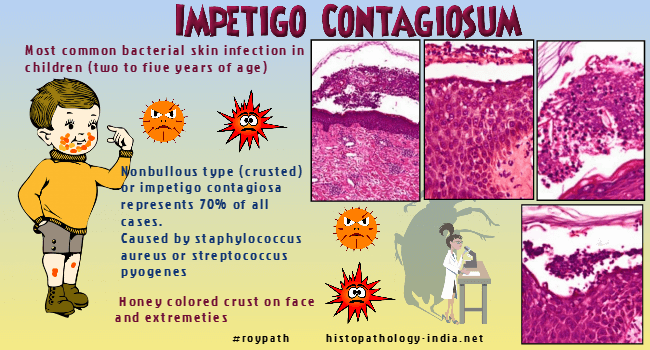
Impetigo is infection of the epidermis
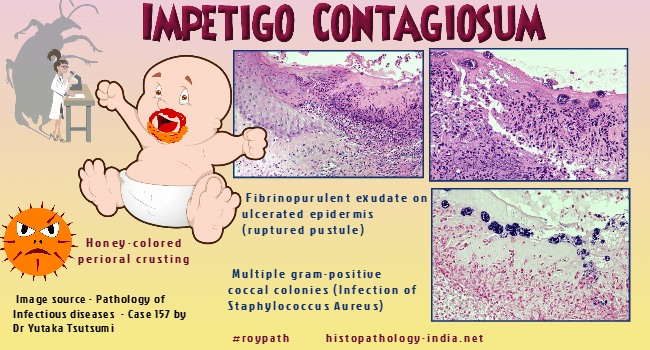
caused by microorganisms. The most common causative organisms are Staphylococcus aureus and group A β haemolytic streptococci (Streptococcus pyogenes). Staphylococcal impetigo frequently affects infants and children. Macular and pustular lesions begin around the nose and spread over the face, forming honey-yellow crusts, the hallmark of impetigo. These crusts are adherent to the surface of the skin, and removal leads to weeping skin lesions. Crusted impetigo can occur in normal skin or may appear over a previous dermatosis such as atopic dermatitis, contact dermatitis, insect bites, pediculosis and scabies. Malnutrition and poor hygiene are predisposing factors. Staphylococcal and streptococcal impetigo exhibit similar lesions, including folliculitis, pyoderma, wound infection, lymphatic spread and sepsis. Staphylococcal impetigo leads to focal tissue necrosis and abscesses more frequently than does streptococcal impetigo. The rarer variant, bullous impetigo, is characterized by fragile fluid-filled vesicles and flaccid blisters and is invariably caused by pathogenic strains of Staphylococcus aureus. Bullous impetigo is at the mild end of a spectrum of blistering skin diseases caused by a staphylococcal exfoliative toxin that, at the other extreme, is represented by widespread painful blistering and superficial denudation (the staphylococcal scalded skin syndrome). In bullous impetigo, the exfoliative toxins are restricted to the area of infection, and bacteria can be cultured from the blister contents. Microscopic features:
Impetigo is rarely biopsied as diagnosis is usually established on clinical grounds. Early lesion is characterized by a subcorneal collection of neutrophils, with exocytosis of these cells through the underlying epidermis. A few acantholytic cells are sometimes seen. In established lesions there is a thick surface crust composed of serum, neutrophils and some parakeratotic material. Gram-positive cocci are found in the surface crust. In bullous impetigo the subcorneal bulla contains a few acantholytic cells together with neutrophils and some Gram-positive cocci. Differential diagnosis: In staphylococcal 'scalded skin' syndrome the exfoliative toxins are spread hematogenously from a localized source causing widespread epidermal damage at distant sites. Both occur more commonly in children under 5 years of age and particularly in neonates. In staphylococcal 'scalded skin' syndrome there is a mild to moderate mixed inflammatory infiltrate in the papillary dermis.
|
|
|

Consultant Histopathologist (Kolkata - India)
|
![]()
Copyright © 2022 histopathology-india.net