

Custom Search
|


| Dermpath-India Pathology of Kimura's Disease
|
|
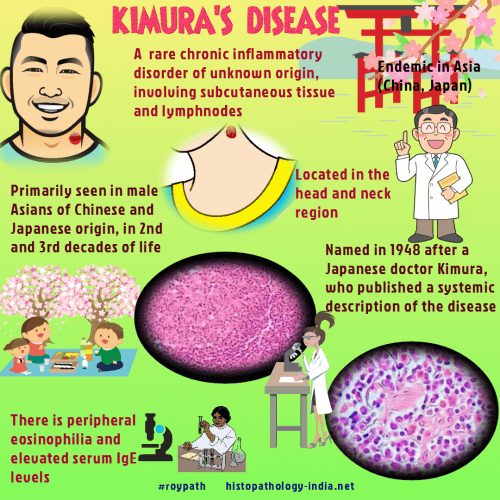
Kimura's disease is a rare,
benign chronic inflammatory condition which commonly occurs among the
Oriental population. It was introduced in China by Kim and Szeto in 1938, but its name was given by Kimura in 1948 from Japan. The exact cause of this disease is unknown but it is believed to result from an immunological reaction that is allergic or autoimmune in nature. The lesion shows no evidence of malignant transformation. Recurrence may occur following surgical excision. Although the Asians are commonly affected some cases have been reported in the Caucasians and in the African population. Age: Usually occurs in the second and third decade of life. Site: Commonly located in the head and neck region particularly in the pre or post auricular region and rarely in the oral mucosa, orbit, and the scalp. Rarely, Kimura's disease may occur in the parotid or other salivary glands. Other rare sites include limbs and trunk, vulva, spermatid cord, inguinal and axillary lymph nodes and peripheral nerves. Clinical presentation: The patient presents with painless subcutaneous nodules or plaques. Lymphadenopathy is present in more than 50% cases. Kimura's disease is often associated with peripheral blood eosinophilia, raised ESR and serum IgE. Accurate diagnosis of Kimura's disease is based on clinical and histological findings. Microscopic features:
Image
Link1 ;
Image Link2;
Image Link3;
Image Link4;
Image Link5. 1. Lymphoid follicles with prominent germinal centre. 2. Fibrous tissue surrounding the lymphoid follicles. 3. Inflammatory cellular infiltrate in the interfollicular area consisting of small lymphocytes, plasma cells and eosinophils. In areas, scattered eosinophilic microabscesses are identified. 4. Thin-walled blood
vessels are increased in number lined by flat or cuboidal endothelial cells. Features of the involved lymph node: 1. Marked hyperplasia of the germinal centre. Germinal centres are often well vascularized and contain eosinophilic deposits and polykaryocytes (Warthin-Finkeldey type). 2. Extensive eosinophilic infiltration consisting of mature eosinophils in follicular and interfollicular areas and occasional eosinophilic microabscess formation. 3. Proliferation of thin-walled blood vessels in the paracortex. 4. Increase in the number
of plasma cells and mast cells in the paracortex. 1.Multiple, small well circumscribed dermal or subcutaneous papules or nodules with well-defined borders. (In Kimura's the lesion is located in the deep soft tissue or the subcutis without significant change of the overlying skin initially ). 2.Less frequently associated with lymphadenopathy and peripheral blood eosinophilia. 3.Histologically, unlike Kimura's disease the blood vessels are lined by plump epithelioid like endothelial cells. These cells demonstrate large nucleus and abundant eosinophilic cytoplasm. Prominent cytoplasmic vacuoles are present. 4.Dense lymphocyic infiltration is present in only some cases of angiolymphoid hyperplasia with eosinophilia.
|
|
|
