

Custom Search
|

|
Infectious Disease Online Pathology of Mycobacterium Avium Intracellulare Infection
|
|
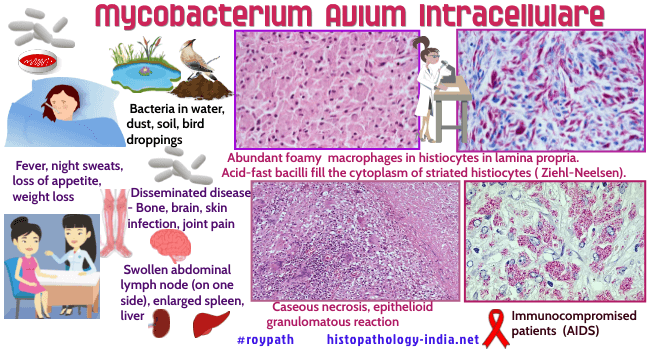
Mycobacterium avium complex
(MAC) include Mycobacterium avium and Mycobacterium intracellulare.
The first probable description of MAC came with the finding of “tuberculosis” in chickens (avian) that mimicked disease seen in humans, described in England in 1868. By 1890, it was recognized that this avian bacteria (now known as Mycobacterium avium) was distinct in the laboratory from the human variety of M. tuberculosis. Human disease due to MAC was not recognized until almost a half century later. In 1933, human-derived disease causing (pathogenic) strains were reported. Later studies revealed the organisms to be M. avium complex. In 1943, one of the first human cases of MAC was described when a mycobacterial species later identified as Mycobacterium avium was recovered from the sputum of a patient suffering from chronic lung disease with an associated underlying lung illness called silicosis (related to silica inhalation). By 1953 (10 years later), more cases of M. avium like organisms in humans were described by other investigators along with four cases that later were identified as M. intracellulare. Mycobacterium avium intracellulare (MAI) is found in the majority of acquired immunodeficiency syndrome (AIDS) patients at necropsy but is only isolated during life in 5-15% of patients with diarrhoea. Disseminated infection is a common pre-terminal event in AIDS patients. Mycobacterium avium intracellulare infection tends to occur late in the course of the disease and in most cases the cause of death is attributable to another infection or process. There are some cases where malabsorption or colitis have been associated with heavy infection with Mycobacterium avium intracellulare as the only isolated potential pathogen. Site: The commonest sites are large bowel, small bowel, liver, oesophagus and associated intra-abdominal lymph nodes but almost no site is exempt from infection. There is evidence to suggest that gastrointestinal infection is the likely early site of colonisation and precedes dissemination. Recent evidence suggests that pulmonary mycobacterium avium intracellulare may also precede dissemination. Endoscopic appearance: May be entirely normal or reveal thickened folds, macular colour changes, plaques or shallow ulceration. Mycobacterium avium intracellulare can be isolated from stool but diagnosis can usually be made on examination of duodenal or colonoscopy biopsy specimens. Microscopic features: Microscopically, Mycobacterium avium intracellulare is characterised by accumulation of abundant foamy macrophages in the lamina propria. These are slender, curvilinear organisms that are sometimes beaded and measure 4-6 micrometer in length. Little or no cellular reaction is noted around the macrophages. The bacilli can also be seen lying free in the lamina propria, presumably as a consequence of disruption to the macrophages. Granuloma formation accompanied by foci of necrosis is seen in those who are immunocompetent whilst those who are immunodeficient, such as AIDS patients, may show subtle pathological changes. In lymph nodes there may be extensive infiltration of the paracortical regions by infected histiocytes. Special stains: The use of the Ziehl-Neelsen stain will reveal infected histiocytes containing numerous intracellular parallel arrays of acid-fast bacilli supporting the routine use of this stain on all biopsies from immunodeficient patients. The organisms stain well with silver impregnation methods. The Mycobacteria are also periodic acid-Schiff (PAS)-positive and diastase-resistant and therefore may be confused with Whipple's disease. Ziehl - Neelsen stain will help to distinguish the two entities. However, culture is also recommended, as histology may not detect small numbers of Mycobacteria. In summary, MAC consists of two species: M. avium and M. intracellulare, which have been recognized for more than 100 years. These two species exist and probably multiply in a wide variety of natural sources including soil, natural and piped water systems, domestic and wild animals, and birds. Some of the environmental strains are similar to those known to cause human disease and because person-to-person transmission has not been confirmed, it seems reasonable to conclude that humans may become infected from the environment.
|
|
|
