

Custom Search
|

|
Infectious Disease Online Pathology of Malaria - Caused by protozoa of the Plasmodium species
|
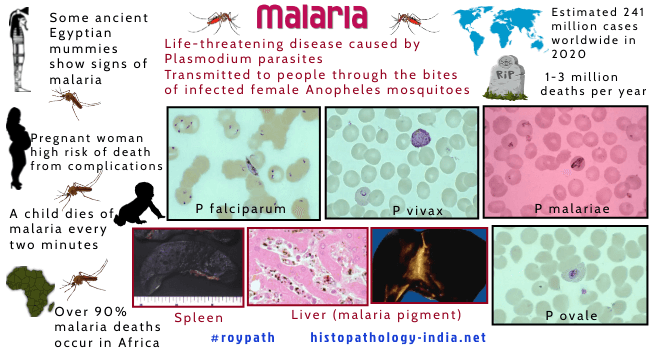
Human malaria is caused by protozoa of the Plasmodium species. It occcurs in any one or a combination of four species of plasmodium - Plasmodium vivex, Plasmodium falciparum, Plasmodium ovale and Plasmodium malariae. Plasmodium falciparum cause malignant tertian malaria with high fatality rate. The other three species are 'benign'. Infections with Plasmodium ovale and Plasmodium malariae are now rare. All forms malaria are transmitted by female anopheles mosquito. WHO recognizes malaria as the world’s major primary health problem. About 2000 million persons suffer from malaria. It is endemic in Asia and Africa but due to widespread jet travel, cases are now reported all over the world. Maternal Malaria: Maternal malaria is a common complication in endemic areas. Plasmodia are found in great numbers in the intervillous spaces of placenta of infected mothers. The parasites sequester along the surface of the placental membrane - trophoblastic villi , extravillous trophoblasts, and syncytial bridges. The sequestration of parasites may obstruct oxygen-nutrient transfer and can cause hemorrhage. The disparity between the approximate 30% incidence of placental malaria in endemic areas and the rarity of congenital malaria reports is believed to be related to an immunologically dependant placental barrier mechanism. In addition to death, maternal malaria is associated with premature delivery, intrauterine growth retardation, perinatal mortality in the infant, and anemia and in the mother. Malaria associated with other Haematological Disorders: The disease has been associated epidemiologically with many hematological disorders. Inherited erythrocyte abnormalities such as sickle hemoglobinopathy and glucose-6-phosphate dehydrogenase deficiency are extremely common in malarial areas. Studies have shown that sickle hemoglobin restricts both parasite invasion and growth. The prevalence of Burkitt's lymphoma in malarious areas has led to the proposal that malaria may enhance the oncogenic potential of the Epstein Barr virus. Life Cycle of Malaria: Female anopheles mosquito sucks patient’s blood containing micro and macrogametocytes (sexual forms). In mosquito, sexual multiplication (Sporogony) produces infective sporozoites in the salivary glands. Mosquito bites a normal person injecting sporozoites into the bloodstream. Some sporozoites leave the blood and enter the hepatocytes where they multiply asexually (exoerythrocytic schizogony) and develops into thousands of uninucleated merozoites. Hepatocyte filled with merozoites are called Schizont. Hepatocytes rupture releasing merozoites into blood. Merozoites enter into RBCs & develop into Trophozoites (ring form). Trophozoite divide to form numerous Schizonts (intraerythrocytic schizogony). Schizonts divide to form merozoites which are released on the rupture of erythrocytes and reenter other erythrocytes to begin a new cycle. After several cycles, subpopulations of merozoites develop into micro and macrogametocytes which are taken up by another mosquito to complete a cycle. Parasitized erythrocytes obstruct capillaries of the brain, heart, kidney and other deep organs. Adherence of parasitized erythrocytes to capillary endothelial cells causes fibrin thrombi which produce microinfarcts. These results in encephalopathy, congestive heart failure, pulmonary edema and frequently death. Ruptured erythrocytes release hemoglobin, erythrocyte debris and malarial pigment. Phagocytosis leads to reticuloendothelial hyperplasia and hepato-splenomegaly. Released hemoglobin produces hemoglobinuric nephrosis (Blackwater fever), which may be fatal.
Malignant Malaria (Plasmodium Falciparum Malaria): Plasmodium falciparum parasites infect liver cells and then red blood cells, cause severe anemia when red blood cell lyse and produce cerebral infarcts when infected red blood cells bind to endothelial cells in the central nervous system. Plasmodium falciparum proteins form unique knobs on the surface of infected red blood cells and parasitised red blood cells adhere to each other and to endothelial cells. Plasmodium falciparum infection initially cause congestion and enlargement of the spleen whereas in chronic malaria infection the spleen becomes increasingly fibrotic and brittle. Pigmented phagocytic cells may be found dispersed throughout the bone marrow, lymph nodes, subcutaneous tissues and lungs. At autopsy the spleen and liver and all organs of reticuloendothelial system in falciform malaria are darkened ("slate grey") by malarial pigment. The hepatic cells show cloudy swelling and fatty change. Kupffer cells are large and actively phagocytic. They contain parasites, erythrocytes and malarial pigment. A disseminated intravascular coagulopathy may occasionally develop in patients with malaria. This has been associated with the adult respiratory distress syndrome seen in some fatal cases of malaria. An immune complex glomerulonephritis formed by Plasmodium falciparum antigen and corresponding antibodies has been documented by electron microscopy and immunofluorescence. Note: Plasmodium falciparum has 37 antigenic variants. Parasites escape cytocidal action of antibodies by altering its antigenic form in circulation. Full protective antibody cannot inactivate the new antigenic variant. As antibodies are formed against this new antigen, parasite changes to yet another variant and this continues till antibodies are formed against all 37 antigens, giving full immunity to infection. This explains why in endemic areas children are subjected to repeated attack of malaria for first few years and then become immune to further infection. Cerebral Malaria: In malignant cerebral malaria caused by Plasmodium falciparum, brain vessels are plugged with parasitized red cells, causing ring hemorrhage. This may be accompanied by necrosis of surrounding parenchyma. Development of trophozoite to schizont takes place in the capillaries of cerebral vessels. Parasitized RBC and are often occluded by microthrombi causing micro-infarct & micro-hemorrhage. The disease starts suddenly or slowly, but rapidly progress to cause impaired consciousness, high fever, chill, generalized convulsions, shock, coma that persists for 24 -72 hours and death within days or weeks. The brain is congested with petechiae limited to white matter. The damage leads to a reactive gliosis with the formation of malarial granulomas (Durck's granuloma ). Differential Diagnosis: i) of ring haemorrhages in the brain: Fat embolism ; bacterial and rickettsial septicaemia ; DIC ; trauma. ii) of pigment containing cells: Formalin pigment. Diagnosis of Malaria: Diagnosis depends on the demonstration of malarial parasites on a Giemsa-stained thick or thin blood smear. Erythrocytes containing multiple ring forms and the presence of banana-shaped gametocytes are diagnostic of Plasmodium falciparum. Because of fluctuations in degree of parasitemia, multiple periodic blood-smear examinations should be performed. The diagnosis can be corroborated by serologic tests. The methods currently available include the indirect hemagglutination antibody (IHA), the ELISA, the indirect fluorescent antibody test (IFA), radioimmunoassay (RIA) and the complement fixation (CF) test. Visit:Blackwater Fever
|
|
|

![]()
Copyright © 2022 histopathology-india.net