

Custom Search
|

|
Infectious Disease Online Pathology of Melioidosis - A Deadly Bacterial Disease
|
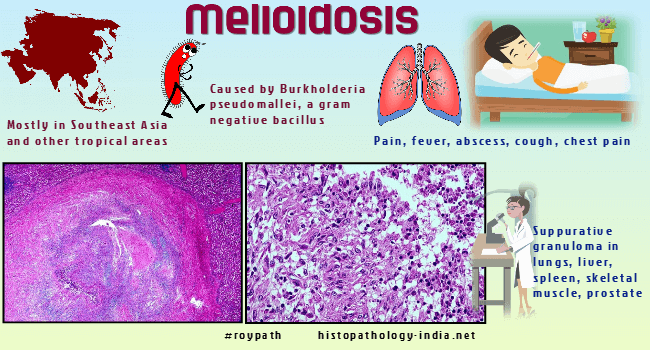
Syn: Rangoon Beggar’s Disease, Vietnamese time bomb and Whitmore’s Disease.Melioidosis is a rare infectious disease caused by Burkholderia pseudomallei, a small gram-negative bacillus in the soil and surface water of Southeast Asia and other tropical areas.Although melioidosis is endemic in Southeast Asia, there have been scattered infections of humans and animals in South and Central America, Africa, Turkey, Australia, and Guam.According to BMJ, India is among the countries at high risk from melioidosis. - India is at high risk from surge in cases of melioidosis, warn researchers During the conflict in Vietnam, several hundred French, Vietnamese and American servicemen acquired melioidosis.The organism flourishes in wet environments, such as rice paddies and marshes.The skin is the usual portal of entry, and organisms enter through preexisting lesions, including penetrating wounds and burns.Man may also be infected by inhaling contaminated dust or aerosolized droplets.The association of melioidosis with drug addiction implies transmission by contaminated needles and syringes.The incubation period varies up to months and possibly years.The clinical course may be chronic, subacute or acute.The acute illness presents as a pulmonary infection, with sudden onset, high fever, chills, malaise, myalgia, and a cough that may produce blood-stained mucopurulent sputum.The severity of pulmonary involvement varies from a mild tracheo-bronchitis to an overwhelming cavitary pneumonia.Splenomegaly, hepatomegaly, and jaundice are sometimes present.The diarrhea may be as severe as in cholera.Fulminating septicemia, shock, coma, and death may develop in spite of antibiotic therapy.Acute septicemic melioidosis causes discrete abscesses throughout the body. These occur most frequently in the lungs, liver, spleen, lymph nodes, and bone marrow, but any organ may be involved. Small, firm, and yellowish lesions are sharply delimited from surrounding normal tissue and are often bounded by a narrow hemorrhagic margin. The small foci may coalesce into larger abscesses. Microscopically, the centers of the abscesses are necrotic and contain neutrophils in a fibrin mesh. A narrow necrotic rim containing histiocytes forms the boundary of the abscess. Necrosis is prominent feature of even the very early lesions, a finding that probably reflects toxin production by Burkholderia pseudomallei. Large numbers of bacteria are seen in the abscesses, but seldom in the surrounding tissue. Subacute melioidosis mimics tuberculosis and is characterized by fever, cough, and pneumonia. Melioidosis also occurs as a self-limited febrile disease lacking specific features. Some 20% of people living in endemic areas have antibodies against Burkholderia pseudomallei. Chronic melioidosis is a localized suppurative infection involving lungs, skin, or bones. Clinically and radiologically it may resemble tuberculosis. Complications include osteomyelitis, psoas or subcutaneous abscesses, and lymphadenopathy. Chronic melioidosis may follow a mild acute illness, or it may lie dormant for months or years, only to appear suddenly- hence the colloquial name , "Vietnamese time bomb". Chronic melioidosis is usually localized to a single organ, most often the lung. The lesions have a necrotic center surrounded by a granulomatous reaction and a perimeter of fibrous tissue. The central necrotic zone may be suppurative or caseous. In the lymph nodes stellate abscesses resemble lesions of lymphogranuloma venereum, cat scratch disease, and tularemia. Bacteria are seldom seen in chronic lesions, even though cultures may be positive. Diagnosis is made by serologic tests or culture. The cultures must be handled carefully, since laboratory-acquired infection is possible. Tetracycline is the treatment of choice.
|
|
|

![]()
Copyright © 2022 histopathology-india.net