

Custom Search
|

|
Infectious Disease Online Pathology of Pneumocystis Pneumonia (Pneumocystis jiroveci pneumonia)
|
| Syn: Pneumocystis Carinii
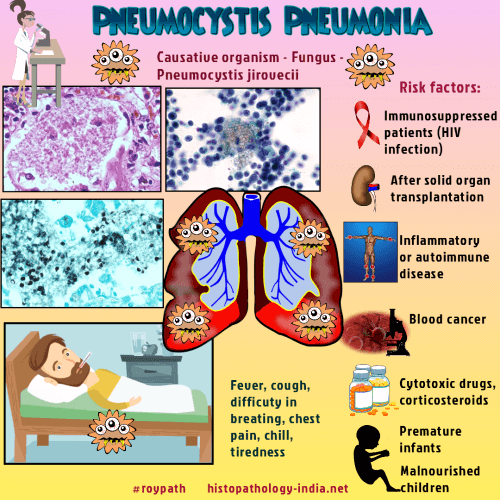
Pneumonia ; Pneumocystosis ; PCP Pneumocystis pneumonia is an endemic or epidemic disease caused by the fungus Pneumocystis jiroveci. The disease used to be called Pneumocystis carinii pneumonia. Pneumocystis organisms from different host species have very different DNA sequences, indicating multiple species. In recognition of its genetic and functional distinctness, the organism that causes human PCP was named Pneumocystis jiroveci Frenkel 1999. Incidence: Present world wide and 75% of population acquire antibody by 5 years of age. Infection occurs by inhalation and most of the infections remain latent. Reactivation with clinical disease is seen only in the setting of severe underlying immunosuppression or overwhelming infection. It is an extremely common cause of infection in patients with AIDS. Pneumocystis infections are also seen in : i) Premature infants. ii) Malnourished children with imperfect immunity. iii) Congenital immune deficiency. iv) Patients- receiving cytotoxic drugs for malignancy, cortocosteroids, & immunosuppressive drugs after transplantation. Concominant infection with other opportunistic organisms such as Aspergillus, Cryptococcus, Candida, and Cytomegalovirus has been reported. Clinical presentation: Fever ; cough ; shortness of breath and less commonly chills and chest pain. Onset of symptoms in immunosuppressed patients may be abrupt and fulminant. In AIDS patients Pneumocystis jiroveci pneumonia seems to present as a more subtle slowly progressive disease illness. Disease in malnourished children has an insidious onset characterized by progressive dyspnea, weight loss and failure to thrive.
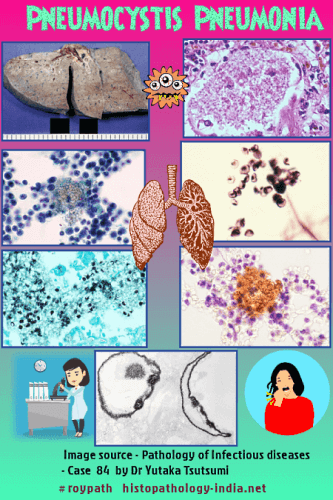
Pathology of Pneumocystis Pneumonia: The infection is largely confined to the lung producing interstitial pneumonia. Rare, but well documented , examples of disseminated pneumocytosis involving the eyes, liver, and spleen have been reported. Gross: Lung is firm, rubbery and noncrepitant. Cut surface may show several firm nodules with a granular mucinous appearance. Nodular areas may be separated by spongy areas of emphysematous pulmonary parenchyma. Microscopic features: 2 stages: Trophozoites and cyst are both present in the pulmonary alveoli. Microscopically, one can identify the small trophozoites (1 to 4 micrometer in diameter) and the larger cysts (8 micrometer in diameter). Hematoxylin and eosin stain shows alveoli which are distended with honey- combed, foamy, brightly eosinophilic material . There is a scanty inflammatory infiltrate composed mainly of monocyte, occasional plasma cells and histiocytes. Special Stains: Grocott's silver stain shows black cysts in alveolar wall and exudates. It looks as round or indented ("new-moon" shape). In Giemsa stain trophozoites are visible in the alveolar exudates (round or crescent shaped & nucleated). Diagnosis: The diagnosis of pneumocystis pneumonia requires microscopical examination in order to identify pneumocystis from a clinically relevant source such as specimens of sputum, bronchoalveolar fluid, or lung tissue, because pneumocystis cannot be cultured. If the initial specimen of induced sputum is negative for pneumocystis, then bronchoscopy with bronchoalveolar lavage should be performed. Transbronchoscopic or surgical lung biopsy is rarely needed. |
|
|

![]()
Copyright © 2021 histopathology-india.net