

Custom Search
|


|
Dermpath-India Pathology of Porocarcinoma Dr Sampurna Roy MD 2022
|
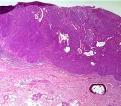
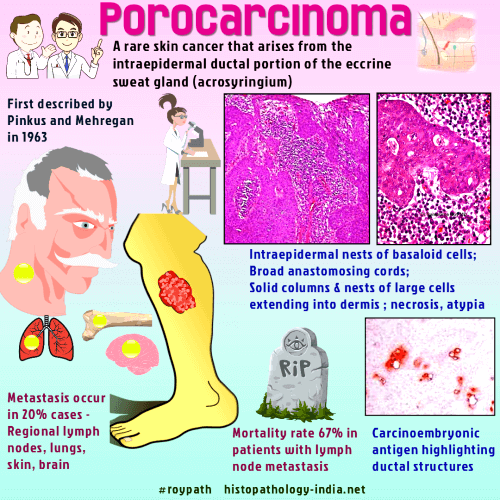

| Porocarcinoma is a rare cutaneous malignancy that arises from the
intraepidermal ductal portion of the eccrine sweat gland (acrosyringium). It was first described, in 1963, by Pinkus and Mehregan as 'epidermotropic eccrine carcinoma' and probably represents the commonest form of sweat gland carcinoma. The name was coined by Mishima and Morioka in 1969. Porocarcinoma may arise denovo , however some tumours are of long duration suggesting malignant transformation of a poroma or hidroacanthoma simplex. ( Hidroacanthoma simplex is a benign eccrine tumor that is also known as intraepidermal poroma.) Age: There is a predilection for older patients and it is often seen during the sixth to eighth decades of life. Sex: It occurs in both sexes. Site: Usually located on distal extremities (44%), followed by the trunk (24%), head (18%), upper limbs (11%), and neck (3%). Clinical presentation: The patient may have a long history of the lesion being present, sometimes up to 50 years. A rapid development of the lesion may occur over a few months. Presents as a verrucous plaque or polypoid growth which may ulcerate or bleed on trauma .
Porocarcinoma tends to be localized. Local recurrence rate is lower than some low grade tumour. Metastasis to local lymphnode may be present in 10-20% of cases. Multiple cutaneous deposits and microscopic epidermotropic deposits may develop. Distant visceral metastases to the lung, retroperitoneum, long bones, breast, liver, mediastinum, urinary bladder, and ovary have been reported.
|
|
Further reading
Metastatic eccrine porocarcinoma: report of a case and review of the literature Eccrine porocarcinoma: a report of 2 cases and review of the literature. Eccrine porocarcinoma: clinical and pathological report of eight cases. Pigmented porocarcinoma: a case report with review of the literature. Eccrine porocarcinoma of the scalp. Eccrine porocarcinoma. A review of 24 cases. Carcinoma of Sweat glands. Pathol Annual. 1987: 22 (part1): 83-124. Sweat gland carcinoma: A comprehensive review. Semin Diagn Pathol. 1987 Feb; 4(1) : 38-74 |
|
|
