

Custom Search
|


| Dermpath-India Pathology of Poroma Dr Sampurna Roy MD 2023
|
 |
|
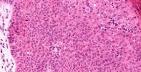
Poroma (poroid tumor) is a benign adnexal tumour that usually originates from the terminal duct of the sweat gland. It is characterised by monomorphous neoplastic epithelial cells that show ductal differentiation. This tumour shows histological overlap with hidradenoma. Initially, in 1956 Pinkus et al. described poroma and its poroid (terminal ductal) differentiation and had been thought to be from the eccrine origin. Further reports have shown cases with apocrine, sebaceous, and follicular differentiation. Previously some authors have grouped them together under the term 'acrospiroma'. Some authors have subdivided Poroma into: Three subtypes of poroid neoplasia in a single lesion: eccrine poroma, hidroacanthoma simplex, and dermal duct tumor. Histologic, histochemical, and ultrastructural findings. 1.Hidroacanthoma group: Hidroacanthoma simplex or intraepidermal poroma (Smith and Coburn 1956) is a form of poroma in which nests of cells with tubular differentiation are confined to surface epidermis. There is no evidence of dermal involvement. Differential diagnosis: Includes melanocytic neoplasm and clonal seborrheic keratosis. Differentiation of hidroacanthoma simplex from clonal seborrheic keratosis-an immuno histochemical study. 2. Poroma group: Intraepidermal and dermal 3. Dermal duct tumour - Intradermal lesion. Poroma containing prominent ductal lumina are known as "Dermal ductal tumour." (Winklemann RK and Mcleod WA 1966). But the tendency, nowadays is to classify all forms as Poroma. Recent analysis suggests that poromas can be of either eccrine or apocrine lineage. Poroma of apocrine lineage are more common. Clinically presents as solitary papule or nodule in elderly patients. Site: Poromas are usually located on the hands and feet . Dermatopathology Quiz Case 143
Related post: Porocarcinoma
|
|
|
|
|
Visit:-
Infectious Disease Online
 Prof (Dr) Haradhan Roy MD (AIIMS) (1928-2022) (R) Director-Professor and Head of the Dept of Pathology, Calcutta National Medical College, Calcutta University India |

Consultant Histopathologist (Kolkata - India)
|
![]()
Copyright © 2002-2023 histopathology-india.net