

Custom Search
|


|
Dermpath-India Cutaneous Lesions in Graft versus Host Disease Dr Sampurna Roy MD 2022
|
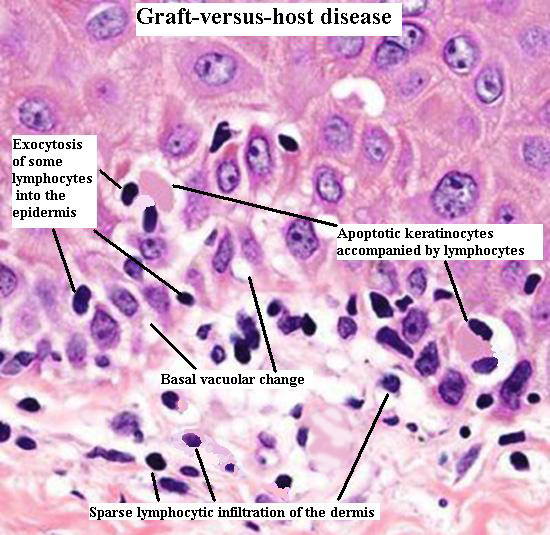
Skin biopsy showing the important microscopic features.
Graft versus host disease occurs in any situation in which immunologically competent cells or their precursors are transplanted into immunologically compromised recipients. (Example- In leukemia, aplastic anaemia and certain immunodeficiency states). GVHD is one of the most important causes of morbidity and mortality following bone marrow transplantation. Early acute phase: Besides the cutaneous lesions, the patient also complains of vomiting, diarrhoea and hepatic dysfuncton. Cutaneous lesions include: - Erythematous macular rash. - Occasionally follicular papules resembling folliculitis. - In severe cases, erythematous to violaceous scaling lesions and even blisters. - Very rarely toxic epidermal necrolysis may occur. Late chronic phase: Chronic phase develops between several months to a year after the transplantation. 1. Early lichenoid phase (both oral and cutaneous lesions clinically resemble lichen planus. 2. Late sclerodermoid phase may be localized or generalized.
Other lesions noted in late phase include esophagitis, liver disease, sicca syndrome, lupus erythematosus-like eruptions, pyogenic granuloma & other angiomatous lesions and alopecia.
|
| Microscopic Features:
There is poor correlation between the
biopsy finding following transplantation and clinical severity of the
disease and biopsy is of limited value in predicting the progression
of the lesion to higher grade GVHD.
Acute Phase: - Sparse, diffuse lymphocytic infiltrate in the upper dermis. - Extensive exocytosis - Basal vacuolation - Scattered shrunken, degenerate keratinocytes throughout the epidermis. - Keratocytes have pyknotic nucleus , eosinophilic and hyalinized cytoplasm and are accompanied by one or more lymphocytes known as "satellite cell necrosis". - In severe cases the appearances are those of toxic epidermal necrolysis. - Differential diagnosis: Subacute radiation dermatitis, drug eruption. Chronic phase: Early lichenoid phase greatly resemble lichen planus - - Acanthosis, - Satellite cell necrosis in the epidermis, - Degeneration of basal cell layer, - Mononuclear cell infiltrate immediately below the epidermis, - Prominent pigment incontinence - In case of follicular papules the features resemble those of lichen planopilaris. - Rarely 'columnar epidermal
necrosis' is noted.
Article
- Atrophy of epidermis. - Basal layer vacuolar degeneration. - Eosinophilic body formation rare or absent. - Thickened or hyalinized collagen bundles which extends into the subcutis.
- Atrophy of adnexal structures due to dermal fibrosis. IgM and C3 in colloid bodies. Granular or linear deposition of IgM in the basement membrane zone is often present.
|
|
|
