

Custom Search
|

|
Infectious Disease Online Pathology of Syphilis
|
|
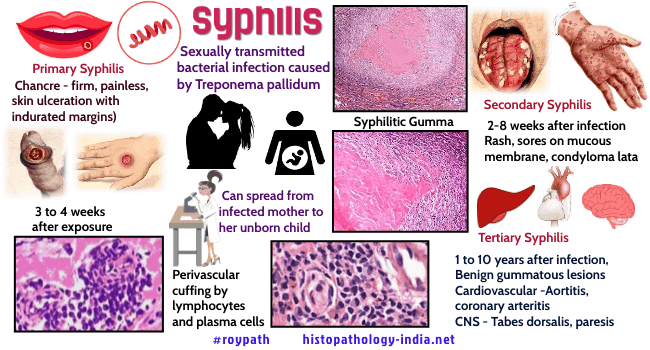
Syphilis, a sexually transmitted disease, caused by the spirochete Treponema pallidum. Historically it was first recognized in Europe in 1490s, and has been related to the return of Christopher Columbus. Mass movements of peoples caused by war and urbanization contributed to its rapid spread. At that time, syphilis was an acute disease that caused destructive skin lesions and early death, but since then it has become milder, with a more protracted and insidious clinical course. The disease is divided into three stages: Primary (the chancre), secondary (disseminated), and tertiary (with lesions of deep organs following a latent period of 2 to 20 years or more). Congenital Syphilis acquired in utero, may have any of the secondary or tertiary lesions. Treponema pallidum is a helical bacterium, 5 to 20 micrometer long and 0.1 to 0.2 micrometer wide, with 8 to 14 evenly distributed coils. The silver impregnation technique precipitates metallic silver on the wall of the spirochete, enlarging its outline and making it opaque, features that make it visible in tissue sections. When smears from chancres or other syphilitic lesions are examined by darkfield microscopy, the spirochetes have the appearance of floating silver-white corkscrews on a black background, spinning on their long axes and flexing in the middle. Various direct and indirect immunoflourescent and immunoperoxidase staining procedures are also available for demonstrating spirochetes in tissue sections and smears. Several serologic and immunoflourescent tests detect organisms, and the host’s antibodies to them. One is the Treponema pallidum immobilization test, in which the live spirochetes of T. pallidum are immobilized by antibody in the patient’s serum. The standard method for demonstrating antibody in the serum is the indirect fluorescent treponemal antibody test, in which the antigen is lyophilized T. pallidum. To increase specificity, nonspecific antibodies in the patients serum are first absorbed by nonpathogenic treponemes. A nontreponemal antigen, cardiolipin from beef heart, is used for diagnostic screening and to assess treatment. Antigenically, it resembles a lipoid released by T. pallidum when it invades human tissues. The Veneral Disease Research Laboratory (VDRL) test and the rapid plasma reagin (RPR) test detect antibodies to cardiolipin. Although useful, these tests are not specific, because lipoidal antigen is released in patients with infectious mononucleosis, viral hepatitis, leprosy and autoimmune diseases. Spirochetes are very fragile and are killed by soap, antiseptics, drying, and cold. Person-to-person transmission requires direct contact between a rich source of spirochetes, for example the chancre, and mucous membranes or abraded skin of the genital organs, rectum, mouth fingers, or nipples. Spirochetes enter the skin or mucous membrane, invade blood and lymph and disseminate almost immediately. Primary Syphilis: The chancre develops at the site of inoculation in 10 to 90 days (average 21 days). It begins as a small papule and may remain a papule. However, when the lesion is large, the chancre develops into a shallow, painless ulcer with indurated margins. The base is covered by fibrin and cellular debris. Spirochetes may be anywhere in the chancre, but they concentrate in the walls of vessels and in the epidermis around the ulcer. Neutrophils migrate into the epithelium around the ulcer, drawn there by spirochetes. The upper dermis is congested and infiltrated with many lymphocytes and plasma cells. Chancres, as well as lesions of secondary, tertiary, and congenital syphilis, have a characteristic “luetic vasculitis”, in which endothelial cells proliferate and swell, and the walls of the vessels become thickened by lymphocytes and fibrous tissue. Early in the vasculitis, lymphocytes are seen in the wall and there may be cuff of plasma cells around the adventitia. Gradually, the inflammatory cells diminish and fibrous tissue replaces the smooth muscle of the media. As the vasculitis continues the lumen narrows, and by the tertiary stage the lumen is reduced to a minute caliber. Spirochetes are visualized in the walls of the vessels in the primary and secondary stages, but not in the tertiary stage. Regional lymph nodes draining the chancre are enlarged and firm, but painless. The chancre disappears in 3 to 12 weeks, and the patient is asymptomatic and immune to reinfection. Secondary Syphilis: Secondary syphilis is characterized by dissemination and lesions in a variety of organs, most strikingly skin, mucous membranes, lymph nodes, stomach, and liver. At first there is a rash that appears 2 weeks to 6 months after the chancre heals. The rash is diffuse, macular, bilateral, and symmetrical and often includes the palms and soles. Next, the mucous membranes of the mouth and the moist genital surfaces display "mucous patches", which develop into shallow ulcers. There are a variety of secondary lesions, including condylomata lata (exudative plaques in the perineum, vulva, or scrotum) ; follicular syphilids (small papular lesions around hair follicles that cause loss of hair) ; and nummular syphilids (coinlike lesions involving the face and perineum). Condylomata lata are characterized by epithelial hyperplasia, acanthosis, infiltrates of plasma cells in the dermis, and a luetic vasculitis. These dermal and mucosal lesions teem with spirochetes. Characteristic changes in lymphnodes include a thickened capsule, follicular hyperplasia, increased numbers of plasma cells, areas of fibrohistiocytic proliferation, clusters of histiocyte encroaching on the germinal centers, and luetic vasculitis. Focal abscesses and scattered granulomas containing giant cells are less common. Numerous spirochetes are present in the walls of vessels, the areas of fibrohistiocytic proliferation, and abscesses. In the secondary syphilis of the stomach, a diffuse infiltrate of the wall by lymphocytes and plasma cells resembles lymphoma. Usually there are numerous spirochetes in the vessel walls and the loose connective tissue. In secondary syphilis of the liver, plasma cells, lymphocytes, and neutrophils infiltrate the portal tracts, in which there is a luetic vasculitis. The serum alkaline phosphatase activity is unusually high. Infections of the meninges begins during the secondary stage and typically persists for life. There may also be optic neuritis during secondary syphilis. The cerebral spinal fluid is abnormal: the lymphocyte count is about 500 per cubic mm (pleocytosis), protein levels are increased, glucose levels are normal, and VDRL tests register positive. The serum likewise is VDRL-positive. Latent SyphilisWhen the lesions of secondary syphilis subside, there is a silent period of “well-being” that lasts for years or decades. However, during this latent period spirochetes continue to multiply, and the deep-seated lesions of tertiary syphilis gradually develop and expand. A few meningeal infections heal spontaneously, but most remain asymptomatic (latent) for years before some are reactivated during tertiary meningeal syphilis. The cerebral spinal fluid shows reduced pleocytosis (about 5 lymphocytes per cubic mm.), and both cerebral spinal fluid and serum are VDRL -positive. During this latent period spirochetes may be passed in blood transfusions or across the placenta to the faetus. Tertiary SyphilisAbout 30% of untreated patients develop tertiary lesions. Syphilitic aortitis, a common tertiary lesion, is characterized by gradual weakening and stretching of the wall of the aorta to form an aneurysm. Grossly, the intima of the aorta appears rough and pitted; it has been described as having the appearance of tree bark. This rough appearance is caused by degeneration of the media, and this in turn is caused by luetic vasculitis of the vasa vasorum. Over the years lumens are gradually narrowed to the point of obliteration, causing ischemia of the wall of the aorta and degeneration of the media. The specialized arrangement of the aortic media, which includes a delicate and intimate weave of elastica, smooth muscle, and collagen, is gradually replaced by scar tissue. It is the specialized tissue of the media that give the aorta its strength and resiliency, and when these are replaced by scar, the aorta gradually stretches, becoming progressively thinner to the point of rupture, massive hemorrhage and sudden death. Damage and scarring of the first part of the aorta commonly lead to stretching of the aortic ring, separation of the aortic cusps and regurgitation through the aortic valve (aortic insufficiency). Syphiliitic vasculitis of the coronary arteries may narrow or occlude the vessels and cause myocardial infarction. The gumma, a characteristic lesion of tertiary syphilis, may form in any organ or tissue. This fibrotic and granulomatous lesion usually presents as an expanding tumour, commonly in the liver and testis. In the liver, there may be a solitary gumma, several large gummas, or widespread small gummas that resembles cirrhosis. Gummas of the testis cause diffuse interstitial fibrosis and contraction of the testis into a round, hard mass. Microscopically, gummas are characterized by a central area of coagulative necrosis, surrounded by epithelioid cells, occasional giant cells, occasional giant cells, and a perimeter of fibrous tissue. The small vessels surrounding the gumma have thick walls and narrow lumens and resemble the vasa vasorum of luetic aortitis. Although infrequently seen, spirochetes are present in the necrotic centers of gummas. Visit - Pathology of Neurosyphilis
|

![]()
Copyright © 2022 histopathology-india.net