Custom Search
|
|
Custom Search
|
|
Dermpath-India Pathology of Digital Papillary Adenocarcinoma Dr Sampurna Roy MD 2022
|
 |
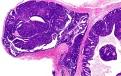
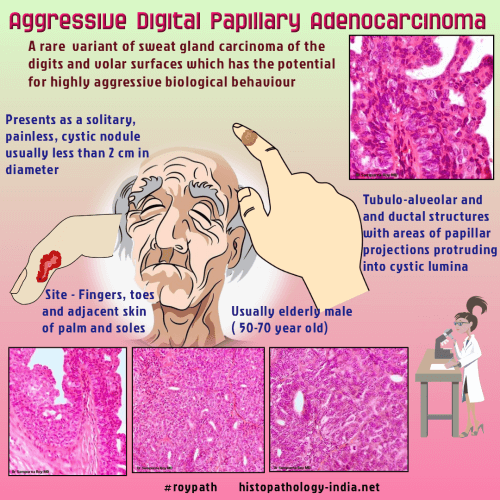
Digital Papillary Adenocarcinoma is a rare variant of sweat gland carcinoma of the digits and volar surfaces which has the potential for highly aggressive biological behaviour. Papillary lesions of the digits were first described in 1987. Based mostly on histologic criteria these lesions were subtyped as: (i) Aggressive digital papillary adenoma. (ii) Aggressive digital papillary adenocarcinoma. Subsequent follow-up has shown that it was not possible to distinguish reliably these two entities. Neither clinical nor histologic features were indicative of biologic behavior of these tumours. Metastatic disease occurred equally with either Aggressive digital papillary adenoma or Aggressive digital papillary adenocarcinoma. The term 'adenoma' was abandoned as all papillary digital neoplasms seemed to have an aggressive behaviour despite benign histologic appearance. Site: Occurs exclusively on fingers, toes and adjacent skin of palms and soles. Clinical presentation: Presents as a solitary, painless, cystic nodule, usually less than 2cm in diameter. Gross features: Tumour has been described as being tan-gray to white-pink and rubbery. [Pathology Infographic]- A Slow growing malignant tumour- Digital Papillary Adenocarcinoma
Recognition of these tumors is important because of a potential risk of local recurrence ( 40 - 50% of patients) and distant metastases (14% of patients), usually involving lymph nodes and/or lungs. Aggressive surgical treatment consisting of wide local excision with clear margins and close surveillance for signs of recurrence or metastasis are indicated for this rare sweat gland neoplasm. Differential diagnosis: May be misdiagnosed particularly for a metastasis of papillary adenocarcinoma originating in the colon, thyroid, or breast. Clinicopathological correlation is essential to rule out a possible risk of metastatic carcinoma of the skin. Papillary Eccrine Adenoma: The ductal structures are larger and more dilated than those in the papillary eccrine adenoma.
|
| Further reading: Aggressive digital papillary adenoma and adenocarcinoma. A clinicopathological study of 57 patients, with histochemical, immunopathological, and ultrastructural observations. Papillary eccrine adenoma should not be mistaken for aggressive digital papillary adenocarcinoma. Aggressive Digital Papillary Adenocarcinoma in a Young Female-a Rare Presentation. Aggressive digital papillary adenocarcinoma diagnosed by fine needle aspiration cytology. Aggressive digital papillary adenocarcinoma: a review. Aggressive digital papillary adenocarcinoma: a report of two diseases and review of the literature. Aggressive digital papillary adenocarcinoma on the palm with pulmonary metastases. Carcinomas of sweat glands. Pathology Annual 22 (Pt 1), 1987; 88-124 . Sweat gland carcinomas: a comprehensive review. Sem Diag Pathol.1987; 4:38-74,
|
|
|
|
|
Visit:-
Infectious Disease Online
![]()
Copyright © 2002-2022 histopathology-india.net