

Custom Search
|

|
Infectious Disease Online Pathology of Mycetoma (Madura Foot ; Maduromycosis)
|
|
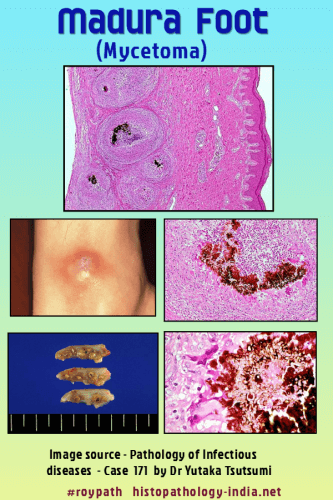
Mycetoma is a localized chronic, and deforming granulomatous infectious disease of subcutaneous tissues, skin and bones, that is present worldwide and endemic in tropical and subtropical regions. It is a pathological process in which the causative agents - a fungus (eumycetoma) or a bacterium (actinomycetoma), from exogenous source produce grains. Distinction between eumycetoma and actinomycetoma is very important for the treatment. Geographic distribution: Seen in tropical region. Example: Asia, Africa, central and south America. Mode of infection: Organisms are normally present in environment (soil and dust). Infection occurs in bare-footed persons after minor penetrating skin injury inoculating soil organisms, occurring preferentially in rural areas, usually among labourers who work barefoot. Age and sex: Mycetoma commonly affects adults aged 20 to 40 years, predominantly males. Site: It is a chronic, tumorous, fungal infection of deep soft tissues and bones of foot (Madura foot). Foot is most commonly affected. Clinical presentation : Both forms of mycetoma present as a progressive, cutaneous and subcutaneous swelling, although actinomycetoma has a more rapid course. Multiple nodules develop which may suppurate and drain through sinuses, discharging grains during the active phase of the disease. Pathological Features: The inflammatory reaction in mycetoma is similar regardless of the causative agent. Visit: Nocardiosis ; Actinomycosis. Lesions contain multiple sinus tracts that usually discharge serosanguinous fluid and, at times, grossly visible granules of various colours, sized, and degrees of hardness depending on the agent involved. Histologically, the dermis and subcutaneous tissue contain localized abscesses, each of which contains one or more granules in its centre. Eosinophilic, clublike Splendore-Hoeppli material may border the granules. Between abscesses, there is extensive formation of granulation tissue, resulting in tumefaction and deformity that is often so severe as to be mistaken clinically for a neoplasm. Infection often involve contiguous bone, resulting in destructive osteomyelitis. Lymphatic or hematogenous dissemination from the primary subcutaneous lesion rarely occurs.
(Adapted from Skin Pathology by Weedon: Pg 675-676.)
Diagnosis : Over 30 species have been identified as causes of mycetoma. The grains of many of these species have overlapping morphological features. Culture is required for accurate identification of the agent. Diagnosis may also involve radiology, ultrasonic imaging, cytology, histology or immunodiagnosis. Identification of the agent is necessary as it guides the mode of treatment. Treatment: Mycetoma caused by bacteria can usually be managed effectively with antibacterial medication alone, while infections with fungi require antifungal medication and surgery. Without proper treatment, mycetoma can lead to deformity, amputation, and death.
|
|
|
