

Custom Search
|

|
Infectious Disease Online Pathology of Paracoccidioidomycosis
|
|
Syn: South
American Blastomycosis.
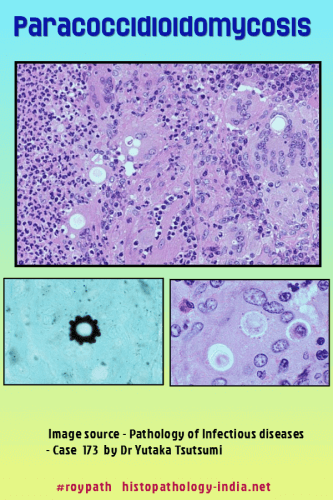
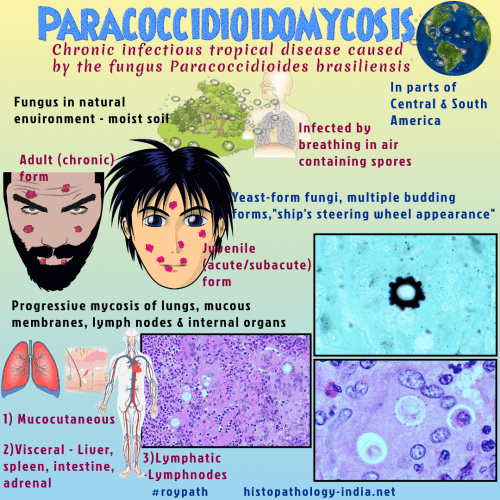
Paracoccidioidomycosis is a systemic mycosis endemic in tropical and subtropical regions of Latin America, due to dimorphic fungi Paracoccidioides brasiliensis and P. lutzii. Geographic distribution: The disease is highly endemic in South America, particularly in Brazil, Colombia, and Venezuela, (coffee growers of Colombia, Venezuela, and Brazil). Cases have also been reported from Central America and Mexico, but cases discovered in the United States have all been acquired within endemic areas of Latin America.
Clinical presentation: Paracoccidioidomycosis is predominantly a disease of rural adult males. Paracoccidioidomycosis infections in women are rare. The primary focus of infection occurs in the lungs, but pulmonary involvement may be overshadowed clinically by manifestations of limited or widespread lymphatic and hematogenous dissemination. Paracoccidioidomycosis of childhood (acute juvenile type) is an acute progressive pulmonary infection that rapidly disseminates to lymph nodes, liver, spleen and bone marrow. It is observed in both sexes and usually presents with adenopathy, hepatosplenomegaly, anemia, diarrhea, and weight loss. The chronic adult type is more common in men older than 35 years of age and in rural workers. It is characterized by skin,mucous membrane, lung, lymph node, and adrenal gland lesions. The adult form that results from reactivation, can cause chronic pulmonary disease with pulmonary fibrosis, emphysema, and bullae. Pathological features: Acute progressive pulmonary paracoccidioidomycosis is an acute suppurative pneumonitis that contains scattered multinucleated giant cells and yeast forms of Paracoccidioides brasiliensis. The chronic progressive form is characterized by granulomatous inflammation with extensive interstitial and conglomerate fibrosis, necrosis, and arterial intimal fibrosis leading to cor pulmonale. At autopsy, disseminated lesions are found in extrathoracic sites in the majority of patients, chiefly involving the oropharyngeal mucosa, larynx, trachea, skin, lymph nodes, liver, spleen, adrenal glands, intestine, and kidneys. The larynx is the third most commonly involved organ in paracoccidioidomycosis. These disseminated lesions are granulomatous or suppurative and granulomatous. Cutaneous and mucosal lesions also exhibit pseudoepitheliomatous hyperplasia similar to that typically found in the lesions of blastomycosis and sporotrichosis. In tissue sections, P. brasiliensis occurs predominantly as pleomorphic yeast-like cells, 5 to 60 micrometer in diameter, that reproduce by budding. Small yeast forms and hyphae are occasionally found. Thick-walled, “mosaic” cells with fractured walls are often numerous in chronic pulmonary lesions. A definitive histopathologic diagnosis of paracoccodioidomycosis requires identification of characteristic multiple-budding cells that resemble a ship’s steering wheel. The blastoconidia produced by these cells have an oval, tubular, or tear-drop configuration and are attached to parent cells by narrow necks. Diagnosis: The precise diagnosis of paracoccidioidomycosis, in most cases, is established by direct methods and indirect immunological tests. The latter method is reliant on the identification of the host's humoral responses, which are usually impaired or absent in patients with severe juvenile forms of the disease and in immunocompromised patients.
|
|
|
