

Custom Search
|

|
Infectious Disease Online Pathology of Respiratory Syncytial Virus Infection
|
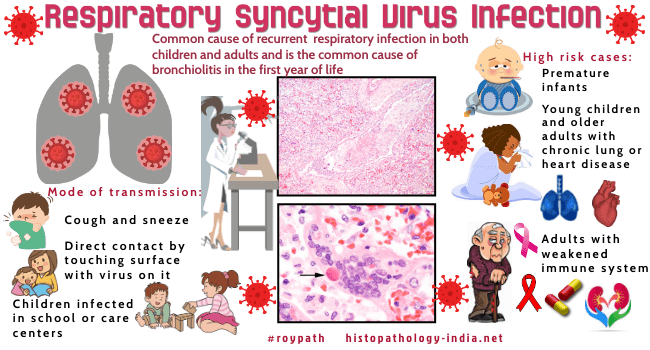
| Respiratory syncytial virus
(RSV) is a common cause of recurrent respiratory infection in both
children and adults and is the leading cause of bronchiolitis in the
first year of life.
|
|
Respiratory syncytial virus (RSV) was first isolated in 1956 by Morris and co-workers who named it "chimpanzee coryza agent". Shortly thereafter, Chanock and co-workers confirmed that the agent was able to cause respiratory illness in humans. Respiratory syncytial virus measures from 121 to 300 nm. It has an RNA genome, and like all members of the paramyxovirus family, the envelop exhibits spokes of glycoprotein. Respiratory syncytial virus is of worldwide distribution, and primary infection occurs in the very young. The majority of children infected with RSV manifest upper respiratory tract symptoms such as rhinitis, cough and coryza. Fever, when present, is usually low-grade. Upper respiratory tract symptoms usually precede lower respiratory tract involvement by a few days.
Pathologic Differential Diagnosis
Herpes simplex and varicella zoster virus rarely produce multinucleated cytologic changes in the lung. Other manifestations of respiratory syncytial virus infection include otitis media, meningitis, myelitis, and myocarditis. Adults at risk of severe disease include immunocompromised hosts, the elderly, and those with pre-existing cardiac and pulmonary diseases. Confirmation of diagnosis is by clinical laboratory tests on immunohistochemistry. Related post: Measles
|
|
|

![]()
Copyright © 2022 histopathology-india.net