

Custom Search
|


|
Dermpath-India Pathology of Clear Cell Sarcoma Dr Sampurna Roy MD 2022
|

|
Syn:
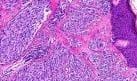
Clear cell sarcoma of tendon and aponeuroses
; malignant
melanoma of soft parts Clear cell sarcoma is a rare aggressive, soft tissue sarcoma which was initially named "malignant melanoma of soft parts".These tumors share histological and immunohistochemical characteristics with malignant melanoma. Unlike malignant melanoma however, most clear cell sarcomas are associated with a t(12;22)(q13-14;q12) translocation. It was originally described by Enzinger et al in 1965. Clear cell sarcoma stain positive for the melanocyte immunohistochemical markers HMB-45 and S-100. It is thought to derive from neural crest cells. These markers are useful for distinguishing clear cell sarcoma from epithelial tumours and synovial sarcomas.
It is a slow growing, progressive tumour with poor prognosis.
The patients are mostly young adults
between the ages of 20 and
40 years with a higher incidence in female.
Poor prognosis is indicated by large size of the tumour , presence of necrosis and local recurrence. Tumors <5 cm are much less likely to recur or metastasize, whereas those >5 cm are more commonly associated with metastatic disease. Focal or diffuse tumor necrosis also correlates with a worse prognosis, independent of tumor size. Metastasis occurs in more than 50% cases. Lymph node metastasis is associated with a poor prognosis, since patients with regional metastasis eventually will develop distant metastasis.
Common sites of metastasis
include bone, lymphnode and lungs. Repeated local recurrence is common
in clear cell sarcoma. The EWS/ATF1 fusion transcript is detectable in almost 90% of cases.
Differential diagnosis of clear cell sarcoma: 1. Malignant melanoma (mitotic activity, cellular atypia and nuclear pleomorphism more prominent in melanoma) Immunohistochemical
studies in
clear cell sarcoma commonly show
neoplastic cells positive with HMB-45, S100 protein, and Melan-A. Most
cases exhibit a t(12;22)(q13;q12) translocation causing an EWSR1/ATF1
gene fusion, a finding that helps differentiate these lesions from
malignant melanoma. 3. Malignant peripheral nerve sheath tumour - Usually arises within large peripheral nerves and is negative for HMB-45. 4. Melanotic Schwannoma, 6. Synovial Sarcoma (monophasic type) - Synovial sarcoma commonly shows a t(X;18)(p11.2;q11.2) translocation producing SYT/SSX1 or SYT/sSSX2 gene fusions, not seen in clear cell sarcoma. 7. Alveolar Soft Part Sarcoma
|
|
|

![]()
Copyright © 2002-2022 histopathology-india.net