

Custom Search
|

|
Infectious Disease Online Pathology of Congenital Syphilis
|
|
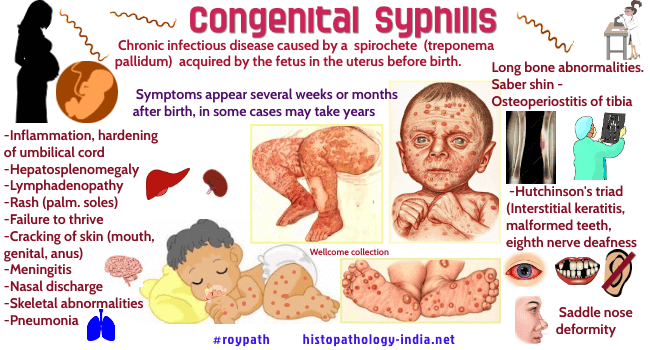
Syphilis may be acquired in utero. The mother becomes infected within 5 years before the pregnancy. Related post: Pathology of Syphilis ; Neurosyphilis ; Bejel ; Yaws After about the fourth month of gestation, spirochetes in the maternal blood cross the placenta and invade the faetus. Infection may cause abortion or stillbirth or may remain inapparent for months or years. Infants also may be infected by contact with maternal lesions at the time of birth. Patients with congenital syphilis have lesions in the skin, mucous membranes, bone, teeth, liver, lung, and central nervous system. The rash may be of any type, including vesicular, bullous, and may be so severe that the epidermis sloughs. Target sites are anus, vulva, palms, soles, and mouth. The dermal vessels show luetic vasculitis and the epidermis teems with spirochetes. Spirochetes invade and grow in many fetal organs and tissues. Damage to bones and reconstruction by periosteum causes two characteristic lesions. The first is a depressed deformity of the bridge of the nose (saddle nose), and the second is anterior bowing of the tibias (saber shins). Infection of the enamel causes notched incisors (Hutchinson’s teeth). In the liver large areas of parenchymal cells are separated by loose fibrous connective tissue (hepar lobatum). Interstitial fibrosis and inflammatory cells in the lung (pneumonia alba) may prevent adequate pulmonary expansion and aeration. Spirochetes may infect the cornea, the optic nerve, and the eighth cranial nerve. Penicillin arrests syphilis in all stages. Tetracycline is given to patients allergic to penicillin.
|
|
|

![]()
Copyright © 2022 histopathology-india.net