

Custom Search
|

|
Infectious Disease Online Pathology of Filariasis
|
| Lymphatic
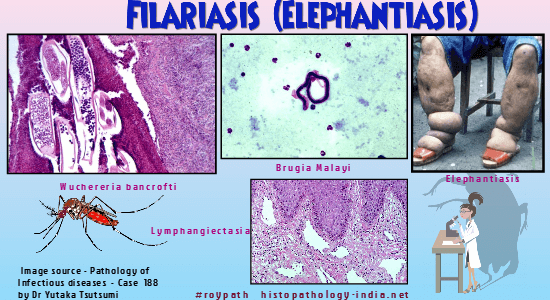
filariasis is transmitted by mosquitoes and is caused by two closely
related nematodes, Wuchereria bancrofti and Brugia malayi.
In Bancroftian filariasis (caused by Wuchereria bancrofti) the mature female worm measures up to 10 cm in length and 3 mm in width, whereas the male is only about one third this size. Geographic distribution: Bancroftian filariasis is endemic in large regions of Africa, coastal areas of Asia, western Pacific islands, and coastal areas and islands of the Carribean basin. Malayan filariasis is endemic in coastal areas of Asia and western Pacific islands. The microfilariae are taken up with the blood of humans by mosquitoes of the genus Culex and occasionally of the genera Aedes and Anopheles. The microfilariae penetrate the stomach wall of the mosquito and reach the thoracic muscles. They undergo multiple changes in the mosquito until they mature and are transmissible to humans. The larva move down to the proboscis of the mosquito, migrate out of the labium, and are implanted on the human skin. They enter the dermal lymphatics and pass to the regional lymph nodes. Maturity occurs either within the lymph nodes or, more frequently, within the larger lymphatic trunks near the regional lymph nodes. The adult worms copulate, and each female worm produces numerous microfilariae. The microfilariae are liberated into the lymphatics and eventually enter the bloodstream, producing a microfilaremia. In the bloodstream they are again available to complete their lifecycle if they are taken up by the mosquito. There is a definite microfilarial periodicity, occurring toward midnight, in most endemic foci. This may be an adaptation to the feeding habits of the vector, which is a night-biting mosquito. A diurnal strain occurs in the South Pacific. Sites involved: The most frequently involved lymphatic vessels are those of the lower limbs, retroperitoneal tissues, spermatic cord, epididymis, retroperitoneal tissues, spermatic cord, epididymis, and mammary gland. The presence of worms in these areas, specially in the region of spermatic cord, does not necessarily imply that the clinical symptoms fever, lymphadenitis, headache and epididymitis will eventually develop. Clinical presentation: (1) Asymptomatic: Most of the patients who are affected remain asymptomatic throughout life. Example: In approximately 20% of autopsies on men in Puerto Rico, histopathologic evidence of filariasis is found in the spermatid cord even though there is no clinical history of the disease. Some patients have massive microfilaremia without the slightest symptoms of the disease. (2) Acute infection: Include fever , lymphangitis , lymphadenitis , orchitis , epididymitis , urticaria , eosinophilia and microfilaremia. (3) Chronic infection: Characterized by enlarged lymph nodes, lymphedema , hydrocele and elephantiasis. Tropical (filarial) eosinophilia: It is also known as Weingartner's syndrome, eosinophilic lung, and tropical pulmonary eosinophilia (TPE ). Tropical (filarial) eosinophilia is a syndrome characterized by cough, wheezing, hypereosinophilia and pulmonary infiltrates. Many patients show impaired lung function with reduction of vital capacity, total lung function, and residual volume. It is believed to be a form of "occult filariasis" that results from hypersensitivity to circulating microfilaria. The term "occult filariasis" has been applied to this condition, as these patients do not demonstrate a microfilaremia on blood smear. A filarial origin can be diagnosed histopathologically when lymph node and other biopsies show trapped microfilariae. A constant and characteristic feature of TPE is peripheral blood hypereosinophilia (3,000-50,000 cells/mm³) in the presence of circulating filarial antibodies. There is an IgE-mediated hypesensitivity to microfilariae in tropical pulmonary eosinophilia. Both IgE and eosinophils may be secondary to secretion of IL-4 and IL-5, respectively, by filaria - specific TH2 helper T-cells. Histopathological examination of organs in Tropical (filarial) eosinophilia : (i) Lung biopsy specimens : Eosinophilic bronchitis and broncho-pneumonia, with multiple small granulomas and areas of necrosis (microabscesses). Foreign body giant cells are common, forming tubercle-like nodules. While intact microfilariae are not generally seen, there may be fragments in the granulomata. The eosinophilic debris, in the form of Splendore-Hoeppli material, implicates helminthic infection. If other organs are biopsied, microfilariae may then be identified. (ii) Liver biopsy specimens: Eosinophilic infiltration along the portal tracts and sinusoids, with associated focal necrosis. Pathologic changes: The pathologic changes in the lymphatics and lymph nodes are attributable to the presence of the adult worm. While the worm is alive, there is minimal reaction on the part of the lymphatics and the most frequent change are those of polypoid endolymphangitis and distension of lymphatics. Death of the adult filarial worm is followed by a severe inflammatory reaction that is characterized by fibrinoid necrosis and pronounced eosinophilic infiltration. The inflammatory reaction develops in nodular fashion around fragmented and necrotic worms. Epithelioid cells and foreign body giant cells appear subsequently. These filarial granulomas are also known a Meyers-Kouvenaar bodies. The filarial granulomas eventually undergo fibrosis, leaving a concentrically lamellated , hyalinized structure that frequently calcifies. Numerous lymphocytes and plasma cells also are seen in the lesion, mostly in the periphery. It is evident from the pathologic processes described that lymphatics will be obstructed and that the severity of this obstruction will depend on the number of worms present. When numerous lymphatics are obliterated by fibrosis, lymphedema results. The classical chronic edema of subcutaneous tissues and the consequent proliferation of fibrous connective tissue and thickening of the epidermis are characteristic of elephantiasis. The full-blown picture of elephantiasis usually develops after repeated episodes of lymphadenitis and ascending lymphangitis. Secondary streptococcal or other type of bacterial infection plays an important role in the pathogenesis of ascending lymphangitis and elephantiasis. In tropical areas the frequency of hydrocele of the tunica vaginalis testis is at least partially related to the incidence of filariasis. The microfilariae only rarely produce visible damage. Occasionally small granulomas, measuring 1 to 2 cm in diameter, are discovered in lymph nodes or spleen, and they may contain microfilariae. The granulomas are composed of proliferating reticuloendothelial cells, fibroblasts and eosinophils. Malayan filariasis is caused by Brugia malayi : A species closely related to W. bancrofti. The pathologic findings are similar to those described for bancroftian filariasis. Pathogenesis of Lymphatic Filariasis: An immunosuppressive state, with altered cell and humoral-mediated immune response, has been reported in patients infected with filariasis. Since lymphatic obstruction is believed to be the result of allergic tissue reactions to the nematode, such immune unresponsiveness would be beneficial to the host and would explain the lack of correlation between infestation and clinical symptoms. Diagnosis: The diagnosis of filariasis is made by identification of the microfilaria on Giemsa-stained blood smears. Blood should be obtained at night because of the periodicity of the microfilaremia. Microfilariae and adult worms are also identified in the tissue sections. Sero-diagnostic methods available are enzyme-linked immunosorbent and indirect hemaglutination tests. Note: The "filarial dance" is a characteristic sonographic appearance that was first described in 1994. This filarial dance refers to random to-and-fro movements of echogenic particles in the epididymis of men infected with W bancrofti. Visit: Onchocerciasis ; Dirofilariasis ; Loiasis:
|
|
|

![]()
Copyright © 2022 histopathology-india.net