Custom Search
|


|
Dermpath-India Pathology of Necrobiosis Lipoidica Dr Sampurna Roy MD 2022
|
| Necrobiosis
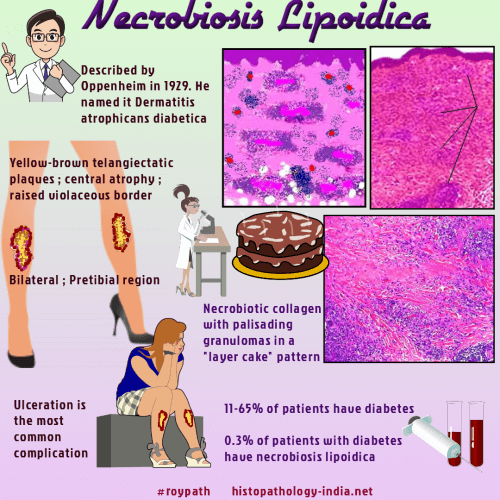
lipoidica , originally known as necrobiosis lipoidica diabeticorum, is a disorder of collagen degeneration with a granulomatous response and
thickening of blood vessels. Diabetes mellitus is present in more than half the patients with necrobiosis lipoidica. Age and sex: Average age of onset is 30 years (may occur at any age) and females are commonly affected. Site: Most cases are located on the leg specially above the tibiae, but may also occur on the face, scalp, forearm and trunk. Clinical presentation: Lesions may be single but multiple lesions are more common. Necrobiosis lipoidica may present as red papules which may enlarge to form patches or plaques with an atrophic yellowish-brown and slightly depressed center. The lesions may resolve spontaneously or become persistent chronic
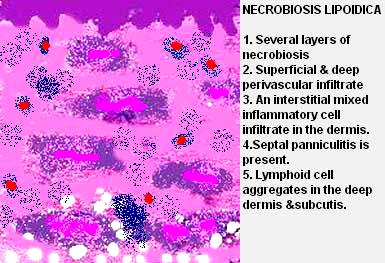
lesions which may ulcerate. Histopathological features: In a fully developed case the characteristic features are present at the edge of the lesion. Necrobiotic granuloma and inflammatory infiltrate: Full thickness of the dermis is involved with extension into the subcutis. The inflammatory cells are composed of histiocytes, lymphocytes, plasma cells and occasional eosinophils are arranged in two or three tiers. These are aligned parallel to the skin surface. There are several layers of necrobiosis within the reticular dermis. Necrobiotic areas are rimmed by histiocytes and multinucleate Langhans or foreign body giant cells. The necrobiosis is irregular and less complete than in granuloma annulare. (Note: Palisaded granuloma in necrobiosis lipoidica- Early lesions show prominent collagen degeneration. Late lesions show crowded and thickened collagen bundles. ) The intervening areas of the dermis are also abnormal. Lymphoid cell aggregates with germinal centers may be present. Abnormalities present in the reticular dermis are also present in the septa of the subcutaneous tissue (septal panniculitis with granulomatous inflammation). Vascular changes: Vascular changes are more prominent in diabetic patients. Superficial and deep perivascular inflammatory infiltrate. Plasma cells are conspicuous. Superficiall vessels are telangiectatic & increased in number. Deeper vessels may show endothelial swelling. Lymphocytic vasculitis may be present. Epithelioid granulomas within or adjacent to the vessel wall.
Other features: Intradermal nerves are reduced in number. Old and atrophic lesions show dermal fibrosis and thickened septa of the subcutaneous fat. Lipid in the upper part of the dermis can be demonstrated by Sudan black and oil red O stain. Stains for mucin (colloidal iron or alcian blue) are usually negative. Differential diagnosis: Interstitial Granulomatous Dermatitis.
|