

Custom Search
|

|
Infectious Disease Online Pathology of Lymphocytic Choriomeningitis
|
|
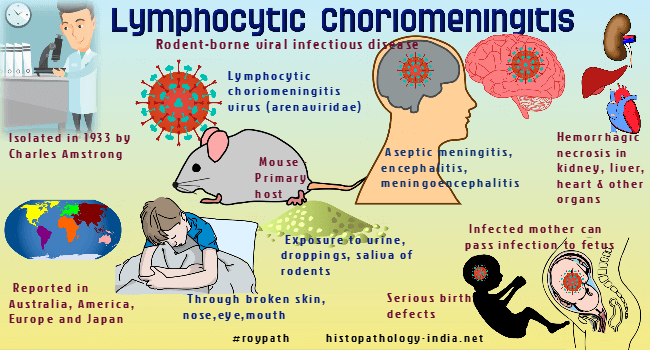
Lymphocytic choriomeningitis, or LCM, is a rodent-borne viral infectious disease that presents as aseptic meningitis (inflammation of the membrane, or meninges, that surrounds the brain and spinal cord), encephalitis (inflammation of the brain), or meningoencephalitis (inflammation of both the brain and meninges). Its causative agent is the lymphocytic choriomeningitis virus (LCMV), a member of the family Arenaviridae that was initially isolated in 1933 by Charles Armstrong. Lymphocytic choriomeningitis (LCM) virus infection is probably widespread through the world, though it has been rigorously documented only in North America and Europe. The mode of spread of lymphocytic choriomeningitis virus in most sporadic human cases is unknown , but studies suggest direct contact with rodents or spread by infected aerosols. The clinical disease produced by lymphocytic choriomeningitis is a meningitis, a meningo-encephalitis, or a self-limited febrile illness. Arthritis, parotiditis, orchitis, and myopericarditis have also been reported. Fatal cases in humans are extremely rare. In monkeys infected by inhalation, virus can be recovered from the lungs and hilar lymphnodes 2 days after infection. Lymphocytic meningitis is often the most conspicuous lesion, but hemorrhagic necrosis may also be seen in liver, kidney, heart, adrenal gland, and other organs. The spleen and lymph nodes show hyperplasia. Congenital Lymphocytic Choriomeningitis Virus Infection: Lymphocytic choriomeningitis virus (LCMV) is an underdiagnosed fetal teratogen. This diagnosis should be considered for infants and children with unexplained hydrocephalus, micro or macrocephaly, intracranial calcifications, chorioretinitis, and nonimmune hydrops. The immunofluorescent antibody test is the only reasonable, commercially available, screening diagnostic tool. The differential diagnosis of congenital Lymphocytic choriomeningitis virus infection includes toxoplasmosis , rubella , cytomegalovirus , herpes simplex virus , enteroviruses, human parvovirus B19 and Syphilis.
|
|
|
