

Custom Search
|


|
Dermpath-India Pathology of Perforating Granuloma Annulare (2022)
|
|
Custom Search
|
|
Dermpath-India Pathology of Perforating Granuloma Annulare (2022)
|
|
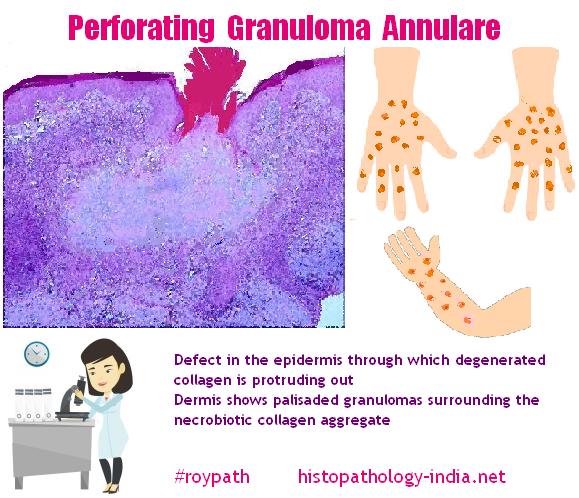
Definition- Perforating granuloma annulare is considered a rare histologic subtype of Granuloma Annulare (GA), with an unknown etiology and chronic course. History- It was first described by Owens and Freeman in 1971. Aetiology- This rare lesion is probably related to delayed hypersensivity, helper T cell response to exogenous antigens. Age, site and clinical presentation Image ; Image ; Image Perforating GA occurs most frequently in children and young adults. A generalized form appears as umbilicated papules that is commonly located on the extremities. Sometimes, progressive stages of the disease can be seen: erythematous papules evolve to yellowish pustular lesions which subsequently discharge a clear fluid. A generalized form characterized by larger plaques with necrobiotic centers, ulceration and crusting could be seen in middle-aged and elderly patients and may be associated with diabetes. Microscopic features- The histopathological features of perforating GA includes the presence of granulomas with histiocytes arranged in a palisading pattern, surrounding necrobiotic collagen. The necrobiotic area is typically represented by deposition of mucin, and rarely fibrin. Often, the histiocytes may become epithelioid and multinucleate and is found phagocytizing elastic fibers. The lesion is often located in the superficial reticular dermis, causing perforation of the acanthotic epidermis and forming a channel for extrusion of degenerated collagen. Special stains such as alcian blue and colloidal iron can be performed to highlight mucin. [Key Microscopic Features: 1) Presence of granulomas with histiocytes arranged in a palisading pattern, surrounding necrobiotic collagen. 2) Necrobiotic area is typically represented by deposition of mucin, and rarely fibrin. 3) Histiocytes may become epithelioid and multinucleate and is found phagocytizing elastic fibers. 4) Lesion located in the superficial reticular dermis, causing perforation of the acanthotic epidermis and forming a channel for extrusion of degenerated collagen. ]
Mechanism of Perforation- The mechanism that leads to perforation is not known. According to some authors the perforation is a result of a transepithelial elimination process. Others suggested that it could represent an epidermal destruction by the superficial granuloma annulare. Some authors have also suggested that the superficial localization of the necrobiotic granuloma and destruction of blood vessels caused by the granuloma could lead to ischaemic epidermal changes that finally cause epidermal destruction. Histopathological Differential Diagnosis - Sarcoidosis and Papulonecrotic Tuberculid- The histopathological differential diagnosis include granulomatous diseases such sarcoidosis or tuberculids as well as perforating dermatoses. Sarcoidosis - The presence of collagen degeneration and multiple palisading granulomas surrounding the necrobiotic collagen without the typical "sarcoidal" granulomas are features more in favour of perforating GA than sarcoidosis. It is important to note that transepithelial elimination could also be present in sarcoidosis. Papulonecrotic tuberculids - These lesions are multiple and arise in symmetric crops and are typically located on the extremities. Histopathologically, the vascular damage is much more intense in papulonecrotic tuberculids than in perforating GA. Histopathological Differential Diagnosis - Perforating dermatoses= Transepithelial elimination, could be present in primary perforating conditions (Reactive Perforating Collagenosis and Elastosis Perforans Serpiginosa), in acquired perforating dermatoses which includes perforating folliculitis, Kyrle disease and acquired perforating collagenosis and in other dermatologic conditions that exhibit transepithelial elimination as an incident histopathologic finding (as in Granuloma Annulare, Necrobiosis Lipoidica , Rheumatoid Nodule and others). Perforating collagenosis usually presents as multiple keratotic papules on the extensor surface of the limbs. Histologically, established lesions of this perforating dermatosis, shows a crateriform depression of the epidermis associated with a keratin plug containing inflammatory debris and collagen fibers. Vertically orientated basophilic collagen fibers are seen in the underlying dermis. Palisading granulomas are not a typical feature. Elastosis perforans serpiginosa has distinct clinical (hyperkeratotic papules grouped in an arciform pattern) and histopathological features (abnormal elastic fibers) which helps in distinguishing this lesion from perforating granuloma annulare. Acquired perforating dermatoses such perforating folliculitis, Kyrle disease and acquired perforating collagenosis have history of an associated systemic disease, as diabetes mellitus, renal failure, liver disease, malignancy or cardiac failure. Unlike perforating folliculitis, in perforating GA, clinically there is absence of folliculocentric papules with a central keratotic plug in hair-bearing areas and histopathologically there is no involvement of the hair follicle.
|
|
|
Visit:- Infectious Disease Online

Consultant Histopathologist (Kolkata - India)
|
![]()
Copyright © 2022 histopathology-india.net